Navigating Chiropractic Frontiers
In this enlightening conversation, we dive deep into Dr. Lona Cook’s chiropractic journey, a chiropractor, coach, author, and visionary leader. Dr. Cook’s impact on chiropractic, her patients, her family, and the world at large is nothing short of inspirational. We listen to her as she shares her experiences from her chiropractic school days to building and scaling successful practices. Additionally, we explore her unique school program, coaching endeavors, and her profound insights on the intersection of chiropractic philosophy, energy awareness, and leadership. Chiropractic Odyssey: From School to Scaling Practices Dr. Cook’s journey began in chiropractic school at Northwestern, an institution with a strong medical orientation. Despite the initial lack of deep philosophical immersion, Dr. Cook’s trajectory took a transformative turn when she attended a New Beginnings seminar. Inspired by Dr. Eddie Diaz’s visualization exercise, she envisioned a world where everyone recognizes the vital role of chiropractic in a child’s health journey. This moment planted the seeds for her future endeavors. Scaling Practices: Fast-forwarding through her successful practice, Dr. Cook emphasized the importance of adapting and pivoting in response to unexpected challenges. While her initial dream was to establish one exceptional practice, she found herself opening a second practice due to personal circumstances. The partnership model, which involved mentoring and a structured buyout, allowed her to scale her practices successfully. Dr. Cook’s insightful perspective on partnerships highlights the significance of alignment, mutual respect, and shared goals for a thriving practice. Philosophical Foundations and Leadership: Dr. Cook delves into the philosophical foundations of chiropractic and the profound impact it has on her leadership philosophy. She emphasizes the importance of understanding metaphysics, epistemology, ethics, politics, and aesthetics—pillars that shape a chiropractor’s worldview. This philosophical depth informs her coaching approach, where leadership transcends mere management. Dr. Cook advocates for cultivating leaders who empower others, creating a ripple effect that extends beyond the chiropractic profession. School Program: Nurturing the Future One of the most captivating aspects of Dr. Cook’s journey is her pioneering school program, bringing chiropractic care to students. Inspired by a New Beginnings seminar, she initiated a program where chiropractors visit schools, initially for teachers and later for students. The program has expanded to multiple schools, with plans to replicate its success in other districts. Dr. Cook envisions a future where chiropractic care becomes an integral part of children’s health and well-being. Energy Awareness and Intuition: Dr. Cook shares her insights on energy awareness, intuition, and their profound impact on decision-making. Drawing from chiropractic philosophy and universal laws, she underscores the importance of recognizing vibrational frequencies in oneself and others. Dr. Cook’s approach aligns with the principle of strengthening strengths and outsourcing weaknesses, fostering a harmonious and impactful leadership style. Coaching with Dr. Cook: Dr. Cook offers coaching services tailored to chiropractors at different stages of their journeys. Prospective clients can initiate the process with a strategy call, where Dr. Cook gains insights into their aspirations and dreams. Her coaching spans from launching and building practices to supporting women in chiropractic who are navigating the complexities of leadership while juggling various roles. Conclusion: Dr. Lona Cook’s chiropractic odyssey is a testament to transformative leadership, aligning philosophy with action, and the profound impact of chiropractic care on individuals and communities. Her visionary initiatives, from scaling practices to pioneering school programs, reflect a commitment to empowering others and leaving a lasting legacy. As we conclude this conversation, Dr. Cook’s words resonate—a reminder that chiropractic is not just a profession; it’s a journey of self-discovery, leadership, and making a difference in the world. View the entire episode by accessing it through: https://bit.ly/3TX5IW7
Optimizing Chiropractic Teams
Today, we’re diving deep into the world of chiropractic hiring with Dr. Mark Mouw, the founder of Chiro Match Makers. Dr. Mouw, a successful clinic owner and coach of The Remarkable Practice, is here to share insights on the challenges of finding the right chiropractic associates and how Chiro Match Makers is transforming the hiring process. Finding the Right Fit: Dr. Mouw kicks off the discussion by emphasizing the critical importance of hiring the right person for the right role to ensure success. With Chiro Match Makers, they have honed in on a strategic approach, utilizing behavioral assessments to identify the best match for chiropractic practices. This is not just about finding any associate but discovering the right fit to achieve long-term synergy. The Evolution of Chiro Match Makers: Dr. Mouw takes us on a journey through the inception of Chiro Match Makers, highlighting the collaborative effort of Dr. Steven France, Dr. Ellen Miner, Sheila, and himself within The Remarkable Practice. Initially focusing on hiring chiropractic assistants (CAs), they soon expanded to include associate searches, addressing a significant need in the profession. Understanding Chiropractic Personalities: The conversation delves into the three main types of chiropractors identified through behavioral assessments: entrepreneurs, business builders, and caregivers. Dr. Mouw breaks down their traits and percentages within the profession. Notably, caregivers make up the majority (65%), seeking fulfilling patient relationships without the desire to run a business. Overcoming Hiring Pitfalls: Dr. Mouw addresses common hiring mistakes, emphasizing the tendency of chiropractors to hire individuals similar to themselves. This leads to challenges when hiring entrepreneurs or business builders who may eventually seek to open their practices, resulting in turnover. Chiro Match Makers aims to shift this paradigm by creating a language of understanding and aligning individuals with complementary traits. The Power of Behavioral Assessments: The Chiro Match Makers team uses licensed behavioral assessments that are EEOC compliant, providing valuable insights into an individual’s behavioral traits. By understanding these traits, practices can strategically build a team that complements each other, fostering a collaborative and successful environment. Scalability and Vision: Dr. Mouw emphasizes the importance of having a clear vision for the practice and building a team that aligns with that vision. The scalability of a practice relies on training, accountability, and autonomy for team members. This approach enables chiropractors to step back from daily operations, promoting long-term stability and durability. Legacy and Exit Strategies: The conversation concludes with insights into legacy-building and exit strategies. Dr. Mouw discusses the four main reasons chiropractors seek assistance: time freedom, increased revenue, stability and durability, and legacy building. Chiro Match Makers and The Remarkable Practice offer comprehensive support, whether it’s finding the right associates or navigating the process of selling a practice. Conclusion: In the dynamic world of chiropractic hiring, Chiro Match Makers and Dr. Mark Mouw stand as beacons of innovation. By incorporating behavioral assessments and strategic insights, they are revolutionizing the way chiropractors build teams and shape the future of their practices. As the profession evolves, finding the right fit becomes not just a necessity but a transformative journey towards success. To watch the full episode, you may view it via: https://bit.ly/48AU07C
Building Empires of Health
In the ever-evolving landscape of healthcare, few stories are as compelling as that of Dr. Jeff Danielson, a chiropractor, visionary entrepreneur, and the mastermind behind Big Fish Enterprises. In an exclusive podcast episode, Dr. Danielson shares the intricate details of his journey, offering listeners a glimpse into the unique blend of chiropractic expertise and business acumen that has propelled him to success. The Genesis of a Visionary: Dr. Jeff Danielson’s story begins in Minneapolis, Minnesota, where he not only thrived as a chiropractor but also cultivated a keen entrepreneurial spirit. It was during his interactions with students at a chiropractic school that he recognized a recurring pattern: young, talented chiropractors eager to make a difference, but often left unsupported after a brief stint in his practice. This realization led to the birth of an innovative coaching program. “Pay It Forward” Philosophy: The heart of Dr. Danielson’s coaching philosophy lies in the concept of “Pay It Forward.” He sought to break the cycle of talented chiropractors leaving after gaining experience and knowledge. Instead, he envisioned a system where associates would be mentored, trained, and ultimately become partners in the journey of acquiring and transforming chiropractic practices. This unique approach has not only benefited Dr. Danielson’s clinics but has created a ripple effect of success through the chiropractic community. Big Fish Training: Transforming Practices: The coaching program, aptly named Big Fish Training, was designed to turn ordinary practices into thriving enterprises. Dr. Danielson emphasizes a hands-on approach, pairing associates with him in his own practice, imparting not just clinical knowledge but the critical skills needed to run a successful chiropractic business. The goal is to transform practices from mere “Ford Taurus” models to high-performance “Lexus” clinics. Team Doc: Revolutionizing Community Engagement: One of Dr. Danielson’s game-changing innovations is Team Doc, a program that redefines community engagement and patient acquisition. By sponsoring local sports teams, especially those in unexpected niches like trap shooting, Dr. Danielson creates opportunities for meaningful connections. This unconventional marketing strategy has proven wildly successful, with dozens of new patients generated from each event, further solidifying the impact of chiropractic care in the community. Chiro Life: A Platform for Transformation: Dr. Jeff Danielson’s commitment to sharing knowledge and fostering collaboration reaches its zenith with the Chiro Life seminar. This annual event is a testament to his vision of building a community of chiropractors who not only excel in their practices but also inspire and support one another. The upcoming seminar, themed “Build Your Army,” promises to be a transformative experience, featuring speakers like Brian Capra, Jeff Langmaid, and Roberto Monaco. Conclusion: Dr. Jeff Danielson’s podcast episode is a masterclass in combining passion, purpose, and business savvy to create a lasting impact in the chiropractic world. His journey, from a chiropractic clinician to a mentor shaping the future of the profession, is an inspiration to aspiring chiropractors and entrepreneurs alike. As the chiropractic community eagerly anticipates the Cairo Life seminar, Dr. Danielson continues to shape the narrative of success in chiropractic care and business. To watch the full episode, you may view it via: https://bit.ly/3TK2qoS
Value Adding for Maximum Profit
I love this topic because it’s easy to miss the mark, especially since so many consultants and marketing firms misappropriate this term and don’t actually coach on value-adding. The idea of value-adding has come under scrutiny in light of the current trend of corporate acquisitions of primary care clinics and the rising patient expectation for comprehensive, patient-centered treatment (Abelson, 2023). This is because of how the healthcare industry is changing. There is a growing need to separate actual value addition from empty rhetoric when corporate companies acquire primary care operations. The demand for genuine, efficient value-adding solutions has never been greater due to the rise in patient expectations for a comprehensive healthcare experience. Don’t get me wrong, plenty do an absolutely amazing job, and their clients see great results, but more often than not, disaster strikes. Especially in the case of Joseph and Bonnie… When Joseph and Bonnie opened their practice, they were die-hard, convinced that they only needed to practice their specialty and nothing else. If we stay true to our specialty’s expertise and principles, we shouldn’t need anything else in the practice to thrive. Although reasonable, this viewpoint failed to consider the changing expectations of healthcare consumers. Patients are increasingly looking for holistic healthcare that covers their current requirements and their long-term well-being, according to Yussof et al. (2022). This suggests Joseph and Bonnie’s single-focused strategy didn’t meet the patient’s desire for comprehensive care. Today’s patients want treatments that address their current health needs and promote wellness, including preventative and long-term health management. Thus, healthcare professionals who offer more services are valued more. So they went about building out a space with the money their mentor had given them and whatever they could find and were adamant that physical therapy was the only service to be offered. Once the space was open, they began marketing to orthopedists in the area and getting patient referrals. That’s when the opportunities opened up. Patients started asking about ancillary services they didn’t have, making them feel like they looked silly. Patients asked about home fitness programs, nutrition, supplementation, and other specialties like Chiropractic or group fitness. The study by Patel & Singhal (2023) demonstrates the growing tendency of patients to seek comprehensive care. It showed that most patients favor healthcare facilities that offer various services under one roof. Patients increasingly view healthcare as a holistic activity. They want nutrition advice, exercise regimens, and alternative cures, not just specialist therapy. This shift in patient preferences fuels the desire for multi-service healthcare facilities that can meet several health and wellness goals. Initially, Joseph and Bonnie ignored it and kept progressing, growing at around 10%. They did a first-quarter review, and it was clear they were not on track to meet their financial freedom goals. They were convinced that something had to change, but they knew working harder to build new referring relationships was not scalable. They could only see so many patients daily, and hiring more therapists would add to their overhead. They needed a solution that minimized overhead growth while maximizing potential revenue. Joseph and Bonnie started taking patient requests seriously and realized a clear pattern. Patients were looking for wellness, not just treatment. Patients wanted to know if they could have a one-stop shop for preventative and therapeutic care. This was a new concept to Joseph and Bonnie, but they began exploring it and found an incredible and vast potential revenue stream in things like product offerings, DME, and more. Such a change toward integrated healthcare delivery is consistent with the ongoing tendency within the pharmaceutical sector to develop into wellness providers with patient-centric services (Moreno, 2019). This represents a larger healthcare shift from treating sickness to promoting well-being. Pharmaceutical corporations are expanding their position to include disease prevention, wellness, and patient-centric services for different health needs. Patients want a single source of preventative and therapeutic care. At first, Joseph and Bonnie only wanted to add what they could manage and keep the specialty singular. However, it soon became clear that their patients were looking for a more sophisticated preventative care so they hired a part-time nutritionist who turned into a full-time nutritionist. They bought used fitness equipment and hired a part-time fitness instructor who turned into a full-time instructor (Joseph recently replaced this person as the full-time trainer because of his personal love of fitness; the perks of being the boss). So what is value adding? Is it simply the addition of multiple complementary specialties into your practice? Maybe. Recent developments in primary and pharmacy care have demonstrated that value addition can be achieved by implementing cutting-edge health methods like digital medicines and remote patient monitoring (Smith, 2021). Value-adding extends beyond incorporating diverse specialties. Digital medicines and remote patient monitoring improve patient care and convenience. These strategies satisfy patients’ desire for individualized, accessible treatment, bringing value to a practice. It could also be the addition of community events, marble floors in the patient bathroom, or a cooling station with fancy refreshments. The true value add in a practice is unique to the patient community. It’s a matter of listening to the value-adds they seek and finding a way to accommodate them that supports the larger purpose and mission. If your practice is in a really nice part of town and you managed to get a great deal on space but are short on cash, it could be a matter of setting up one fancy area in your practice that you can afford to spruce up (it should also be functional, before you go replacing drapes). Whatever change you attempt needs to address two things: Patient requests – Surveys often help the most in this area Patient function – You want the value to add(s) to be usable in some way that improves the patient’s experience both individually and as a group A fancy cooling station with multiple settings, fruit, vegetable-enhanced water, and more can get patients talking and feeling fancy. Often these changes can also help enhance the practice’s
Maximizing Chiropractic Efficiency: The Power of Integrated Software Solutions
In today’s digital age, the healthcare industry, including chiropractic practices, is rapidly evolving. With the rise of technology, there’s an increasing need for integrated software solutions that can streamline operations, enhance patient experience, and boost overall efficiency. In this context, the integration of platforms like Genesis Chiropractic Software and TrackStat is nothing short of revolutionary. The Need for Automation in Chiropractic Practices Automation is no longer a luxury but a necessity. With the increasing demands on healthcare professionals, manual processes can become tedious and prone to errors. By automating tasks such as patient management, appointment scheduling, and follow-ups, chiropractors can ensure a smoother and more efficient workflow. This not only saves time but also reduces the chances of human error, ensuring that patients receive consistent and high-quality care. Segmentation for Personalized Patient Care One size doesn’t fit all, especially in healthcare. Every patient is unique, with different needs and health conditions. By segmenting patients into different categories based on their health conditions, treatment plans, or other criteria, chiropractors can offer more personalized care. This not only enhances the patient experience but also ensures that each patient receives the most appropriate and effective treatment. The Power of Sales Pipelines in Patient Conversion A robust sales pipeline is crucial for any business, including chiropractic practices. By tracking new patients, their last and next visits, and other relevant information, chiropractors can gain valuable insights into their conversion rates. This data can be instrumental in identifying areas of improvement and implementing strategies to boost patient conversion. Enhancing Patient Retention with Data Analytics Patient retention is a critical metric for any healthcare practice. By analyzing data on patient drop-offs, chiropractors can identify specific points in the patient journey where they’re losing patients. With this information in hand, they can implement targeted strategies, such as educational workshops or progress exams, to enhance patient retention. Streamlining Operations with Two-Way Texting and Smart Reactivations Communication is key in healthcare. Two-way texting allows for seamless communication between chiropractors and their patients, ensuring that patients are always informed and engaged. Additionally, smart reactivations can help chiropractors identify and reach out to patients who haven’t been in for a while, ensuring that they continue to receive the care they need. Reducing Accounts Receivable with Integrated Solutions Financial health is crucial for the sustainability of any practice. By integrating solutions that help reduce accounts receivable, chiropractors can ensure a steady cash flow and financial stability. This not only ensures the smooth running of the practice but also allows chiropractors to invest in further enhancing their services. Conclusion The integration of platforms like Genesis Chiropractic Software and TrackStat offers a plethora of benefits for chiropractic practices. From automating tasks to enhancing patient experience and boosting efficiency, these integrated solutions are truly game-changers. As the healthcare industry continues to evolve, it’s crucial for chiropractors to leverage the power of technology to stay ahead of the curve and offer the best possible care to their patients. Note: For a deeper dive into these topics and to hear firsthand experiences from industry experts, watch the video at the top of this page.
Why ClinicMind?
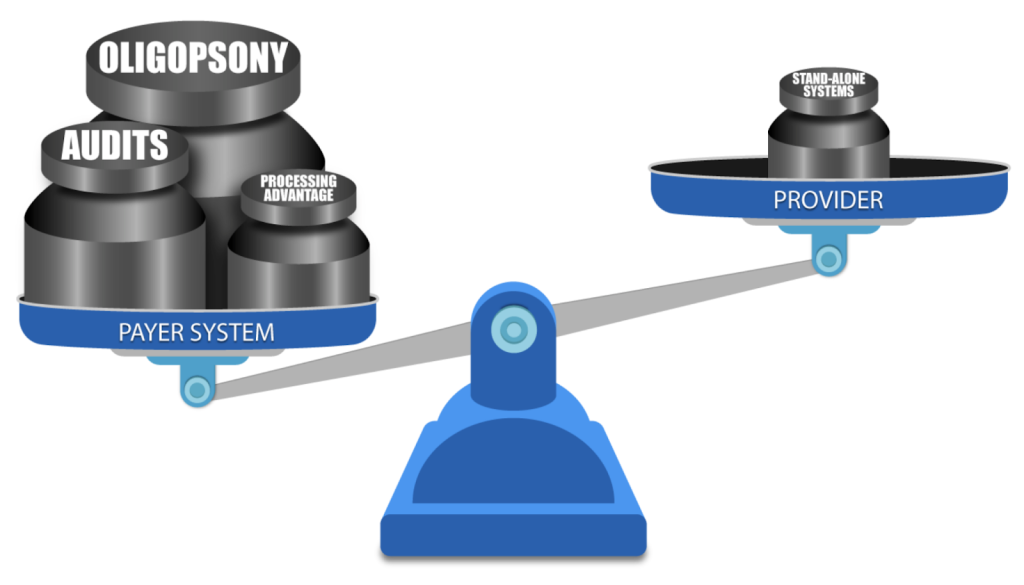
DO YOU know a practice owner who wants more patients in her clinic, better pay-per-visit, and better collections? We all know healthcare practice owners who want to remain independent and grow and yet are frustrated by insurance companies and continuous battles to get paid and stay compliant. Now, as a patient, do you like visiting a healthcare practice, receiving bills, and reconciling them with your insurance company? You are not alone. As it turns out, most other people do not like their patient experience. The problem is that patient and independent practice needs have evolved in step with society and technology, but management methodology remained in the 19th century. There’s a fundamental mismatch between how healthcare practices and patients are managed — and the practice owners’ and patients’ expectations. We came to a startling observation: patients no longer want their care to be managed the way it used to be managed in the previous century. And yet, practice owners still use their old methods to memory-manage their practice. Who is taking advantage of this mismatch? The insurance companies – payers. From the outset, we knew that healthcare costs are spiraling out of control. We also knew that insurance companies, medical equipment manufacturers, pharmaceuticals, and hospital executives have been all making handsome returns and benefitting from healthcare cost growth. One question bothered us: why are the practice owners unable to participate in that growth? How was it that the key contributors to healthcare service were excluded from fair compensation for their work and grew exceedingly frustrated with rules and regulations? Some providers were selling their practices to join larger networks or hospitals, and others were moving to different industries. National studies have shown that physician burnout rates are climbing up. For instance, Mayo Clinic Proceedings reported that the prevalence of burnout among U.S. physicians was 63% in 2021, compared with 38% in 2020, 44% in 2017, 54% in 2014, and 46% in 2011. We also noticed that with experience, medical billing managers start cherry-picking insurance companies for easy follow-up. So, the practice owners could not get paid on time and in full by a growing number of insurance companies (payers). The more obstacles payers pose – the less paid the providers are. Payers were stacking the game against the providers by continuously adding new rules to reduce payments and increasing the frequency of provider audits. In addition to continuous consolidation, resulting in scarcity of payers (a market structure known in economics as Oligopsony), which allows the payers to drive the reimbursement fees down, they also have a two-pronged resource advantage: attract Ivy-league MBAs to build sophisticated claim-processing protocols and discover every little pretext to deny or delay claim payment leverage the most powerful digital technology to implement those protocols on the ever-growing volume of claims. ClinicMind was founded to address two basic challenges facing providers: a patient-provider expectations mismatch and payer-provider adversity. First, the patients have transformed how they expect healthcare service delivery, but practice owners have not adapted their practice management methodology. Second, insurance payers underpay and delay payments because they make a substantial profit from the “float.” The float is the money insurers hold onto between the time they collect premiums and the time they pay out claims. In summary, 1. The Basic Mismatch Between Patients and Providers: a. Background: The healthcare industry has undergone significant changes in recent years, with patients becoming more proactive in managing their healthcare and demanding a different level of service. This transformation is largely due to increased access to health information through the Internet and the rise of patient-centered care models. However, many practice owners, particularly in traditional healthcare settings, have not adapted their practice management methodology to meet these changing patient expectations. b. Conflict: Patient Expectations: Patients today expect convenience, transparency, and a more personalized approach to healthcare. They want to schedule appointments online, access their medical records easily, and receive timely, clear communication from their healthcare providers. Provider Resistance: Many practice owners and healthcare providers are accustomed to traditional, paper-based methods and may hesitate to embrace digital technologies or change their established processes. This resistance can result from the comfort with the status quo, fear of the unknown, or high implementation costs. c. Resolution: To resolve this conflict, healthcare practices must adapt to the changing landscape. This may involve investing in electronic health records (EHR) systems, online appointment scheduling, telemedicine services, and more. Additionally, training staff and providers to use these technologies effectively is crucial. Clear communication with patients about these changes, the benefits they bring, and how data security and privacy are maintained can help build trust and reduce resistance. 2. Payer-Provider Adversity: a. Background: In the healthcare system, insurance payers (such as health insurance companies) often maintain a substantial portion of their profit through a financial mechanism called the “float.” The float is the money insurers hold onto between the time they collect premiums and the time they pay out claims. This float can represent a significant source of income for payers. However, it can create a conflict of interest with healthcare providers. b. Conflict: Payer Profit: Insurance payers benefit from maintaining a healthy float, as they can invest these funds and earn returns. The larger the float, the more profit they can potentially make. Payers have a significant advantage over the providers because of the oligopsony and because of significantly larger resources for better talent hiring and data processing. Provider Concerns: Healthcare providers, on the other hand, often face challenges in receiving timely and appropriate payments from payers. Delays or disputes in claims processing can impact their cash flow and ability to provide care. Providers feel that payers prioritize maintaining their float over ensuring prompt reimbursement. c. Resolution: Transparency and fair contracting: Establish clear and fair contracts between payers and providers that outline payment terms, including prompt payment schedules and dispute resolution mechanisms. Industry consolidation: Metcalf’s Law states that the value of a network is
Leading with Purpose: Resilience and Revolution in Chiropractic Care with Dr. Gilles LaMarche!
In the vast landscape of healthcare, chiropractic care often occupies a misunderstood and underutilized corner. Yet, this specialized field has so much to offer, not only in terms of physical wellness but overall health and vitality. This article sheds light on the broader implications of chiropractic practice, inspired by the profound insights shared by chiropractic trailblazer, Dr. Gilles LaMarche. The Chiropractic Paradigm: A Game-Changer for Health The nervous system, with its extensive network of nerves and cells, serves as the body’s primary system. It is the master controller of our body, orchestrating each function and process. Yet, many of us overlook its role in our health journey. A chiropractic approach places the nervous system at the forefront, emphasizing the importance of maintaining its optimal function to achieve overall well-being. Chiropractic care transcends beyond addressing neck and back pain—it is about unlocking the body’s potential to self-heal and self-regulate. As more people begin to grasp this, they can make more informed decisions about their health, prioritizing spinal and neurological health as essential aspects of their wellness routine. Young Chiropractors: The Future Advocates As the healthcare paradigm shifts towards prevention and holistic well-being, it’s an opportune moment for young chiropractors to step forward. They can be the advocates for change, sharing their expertise in neurological function and spinal health with the broader healthcare community and their local circles of influence. Even the smallest communities can benefit from their visibility, gradually erasing misconceptions and elevating the understanding of chiropractic care. Authorship as Influence Credibility is key in the information-saturated world we live in. For chiropractors, writing and publishing work on chiropractic practice can elevate their standing in the community, while also expanding their reach. Dr. LaMarche’s own experience as an author has seen the beneficial effects of such endeavours, with chiropractors being able to enlighten more people about the benefits of chiropractic care through their published works. As we move forward in an era where personalized, holistic health care becomes the norm, chiropractic care is poised to play a significant role. The insights from Dr. Gilles LaMarche underline the potential of chiropractors as essential health providers and advocates for change, propelling us towards a future where spinal health and well-being are recognized for the pivotal roles they play in our overall health. It’s time to unleash the full power of chiropractic.
Decoding Success: A Deep Dive into Thriving in the Chiropractic Business
Welcome to our latest discussion on the ins and outs of the chiropractic business world. Today, we’re bringing you the key insights from a riveting conversation between Dr. Brian Paris, a prominent figure at Genesis Chiropractic Software, and Jeff Van Kampen, the go-to expert at Clinic Growth Accelerator. They’ve generously shared their wisdom on what it takes to prosper in today’s ever-evolving chiropractic industry. Understanding Your Position Starting a chiropractic business isn’t all sunshine and roses – it requires a deep understanding of your market positioning. As Jeff articulates, a chiropractor beginning their journey shouldn’t compare themselves to established brands like Ritz Carlton or Nike. These big names have had years to build their brand, starting from scratch just like any other business. Your practice might be offering the highest quality services in town, but remember – building a brand takes time, capital, and strategy. As Jeff puts it, if you’re just starting out, look at how these successful brands operated when they began, not at their current standing. The Power of Direct Response Advertising When you’re starting, Jeff suggests investing in direct response advertising. This form of advertising targets individuals who are ready to take action, providing an immediate return on investment. But it’s not just about immediate returns; you’re also building a list. Suppose you spend a substantial sum on chiropractic Facebook ads. Not only are you attracting potential patients, but you’re also creating a valuable list of local individuals interested in chiropractic services. This list becomes a long-term asset that can be leveraged for email marketing, text marketing, and outbound cold calls, helping you craft effective and targeted marketing campaigns. Streamline Your Processes According to Dr. Brian, the biggest gap in many chiropractic businesses is inconsistency in their processes. Having a structured, systematic approach to every step – from patient check-ins to reexaminations and teaching rehab exercises – is critical to your business’s success. Having a clear process helps you identify bottlenecks in your operations. If everything is left to chance, identifying these hindrances becomes virtually impossible. For instance, if a staff member tasked with office tours isn’t performing optimally, a systematic approach would help you quickly identify and address the issue. Identify Your Main Bottleneck Speaking of bottlenecks, Jeff argues that at any given time, your business will have one primary bottleneck. This bottleneck might be in sales, marketing, or your team – but there’s always just one main obstacle preventing further growth. Identifying and resolving this bottleneck is crucial for your business’s evolution. Building Relationships Finally, the conversation underscores the importance of building relationships, both with clients and within the industry. Whether it’s maintaining a casual rapport with clients or establishing strategic partnerships like the one between Genesis and Clinic Growth Accelerator, nurturing relationships is a cornerstone of success in the chiropractic industry. The insights shared by Dr. Brian Paris and Jeff Van Kampen shine a spotlight on the core aspects of successfully running a chiropractic business. As the journey from seven to eight figures unfolds, we can look forward to more wisdom, more lessons, and more growth. Stay tuned!
The Future of Chiropractic: Overcoming Challenges and Embracing Opportunities
In the ever-evolving landscape of healthcare, the chiropractic profession finds itself at an intersection of significant opportunities and formidable challenges. Our recent interview between Dr. Brian Paris from Genesis Chiropractic Software and Bharon Hoag, a prominent advocate for chiropractic illuminates the profession’s enormous potential and its concurrent hurdles. Legal Challenges: A Global Concern The chiropractic profession’s legal battles are not confined to the United States but are truly a global concern. The battles fought internationally are critical to the defense and evolution of chiropractic. Proactively confronting these issues at their onset in other countries serves as a preventative measure to protect the profession in the U.S., effectively circumventing the development of more intricate and expensive legal predicaments. Hoag underscored that out of approximately 700 legal battles they engaged with, around 660 occurred outside of the United States. This strategic approach to legal challenges ensures that potential threats to the profession are intercepted and addressed before they reach the home turf, where their impact could be more detrimental. The Power of Collaboration in Chiropractic Arguably one of the most essential insights from Hoag’s conversation with Dr. Paris is the emphasis on collaboration over competition. The future of the chiropractic profession will not be defined by infighting or territorial disputes among different organizations within the profession but by their capacity to work cohesively for the common goal: advancing chiropractic practice. Hoag highlighted the importance of understanding that each organization has a distinct role to play in the larger chiropractic ecosystem. By acknowledging and respecting these differences, organizations can coexist and collaborate effectively, thus bolstering the collective strength of the profession. Embracing Growth: Increasing Support and Resources To confront the emerging challenges effectively and capitalize on the burgeoning opportunities, the chiropractic profession needs to embrace growth—not merely in numbers, but in terms of resources and support. Hoag stressed that the focus shouldn’t be on soliciting large contributions that require significant fundraising efforts. Instead, the goal is to garner support from a broad base of contributors who can collectively provide the resources needed to meet the profession’s growing needs. Hoag aims to rally 10,000 contributors to meet the profession’s needs. With more resources, the profession will be better equipped to respond to growing demands, defend itself in legal battles, and continue to make strides in the wider healthcare landscape. Nurturing the Future of Chiropractic An enduring commitment to the profession’s future is clearly evident in Hoag’s narrative. Preparing the next generation of chiropractic professionals to take up the mantle is a crucial element of this commitment. Hoag, whose own children are stepping into the profession, stressed the need for creating a profession that young practitioners can not only be a part of but also take pride in. The upcoming generation of chiropractors is passionate, skilled, and poised to make a significant difference in healthcare. It is incumbent upon the current leaders of the profession to foster an environment that nurtures these aspirants’ potential and passion. Chiropractic’s Role in Integrated Healthcare At its core, the chiropractic profession has the potential to instigate a transformative shift in our healthcare system. By advocating for the integration of chiropractic into mainstream healthcare, we can instigate a new approach to health and wellness that prizes natural healing methods. Hoag believes that this integration can not only dramatically improve individual health outcomes but can also significantly influence the economic structure and enhance human interactions globally. This potential extends from the micro-level, where practitioners engage personally with patients, to the macro-level, where systemic change can redefine the healthcare landscape. Visit the Chiropractic Defense Council here
Implementing EOS: Cultivating Success and Collaboration in the Chiropractic Profession
The chiropractic profession is a rapidly evolving field, brimming with passion, creativity, and a drive to heal. However, these strengths often come hand-in-hand with challenges in business operation and growth. To propel the industry forward, chiropractors are increasingly realizing the need to apply systematic, strategic approaches to their businesses. One solution that’s gaining traction is the Entrepreneurial Operating System (EOS), a holistic business management system that focuses on aligning team vision and creating processes for more efficient, effective work. EOS coach Jill, from EOS Worldwide, and Dr. Brian Paris recently sat down to discuss the role of EOS in improving chiropractic practices. They dived into the nuts and bolts of the EOS process and how it can support businesses to flourish in the complex healthcare marketplace. The EOS System in Practice One of the crucial aspects of the EOS system is its emphasis on simplifying complex structures. At its core, EOS is about stripping down complicated processes to the bare bones, helping businesses identify their unique strengths and weaknesses. Jill emphasized the importance of developing a clear, shared vision within the chiropractic business. She noted that common pitfalls for practices include a lack of clarity and unity in their team’s vision. EOS aims to create a cohesive, productive team environment where everyone is in sync and working toward a common goal. She also discussed the concept of the Entrepreneurial Range, a spectrum ranging from a ‘true entrepreneur’ to a ‘true manager’. Understanding where individuals lie on this spectrum, she says, allows for optimal team alignment and, ultimately, business success. Challenging the Norms: Confronting Complacency and Embracing Pain Dr. Brian argued that complacency, rather than struggle, is detrimental to a business’s growth. The belief that operating a business without pain or discomfort is desirable or achievable can often lead to stagnation. By contrast, embracing difficulties as necessary for growth can catalyze meaningful progress and evolution. With the right business tools and strategies, the pain of change can give way to a place of freedom, creativity, and successful operation. Cultivating Collaboration over Competition The pair also stressed the significance of a collaborative approach within the profession. By viewing other practitioners not as competition but as potential sources of knowledge and growth, chiropractors can create a more unified and stronger industry. This mindset can extend to shared challenges, such as dealing with insurance companies and politics, where collective strength and unity are beneficial. Harnessing the Power of EOS: A Success Story Jill shared a success story of a roofing client who, through EOS implementation, transitioned from a stagnant business to a thriving enterprise making a global impact. By buying out a non-compatible partner, hiring an integrator, and simplifying their business model, they transformed their operation. They’re now winning awards and using their resources to contribute positively to global communities. This example highlights how EOS can help businesses expand beyond their initial self-conception, creating growth opportunities and making a difference at a larger scale. It serves as an inspiration for chiropractic businesses seeking to redefine their own boundaries and potential. Conclusion: EOS for the Future of the Chiropractic Profession The chiropractic profession stands to benefit significantly from strategic business models like EOS. By fostering clear vision, embracing challenges, and cultivating collaboration, EOS can empower chiropractic businesses to thrive in an ever-changing healthcare landscape. For any chiropractor contemplating leveraging a coach, it’s important to remember that the goal is to get everything you want out of your business while living your ideal life. And, as Jill has shown, EOS could well be the path to that goal.
