Justified
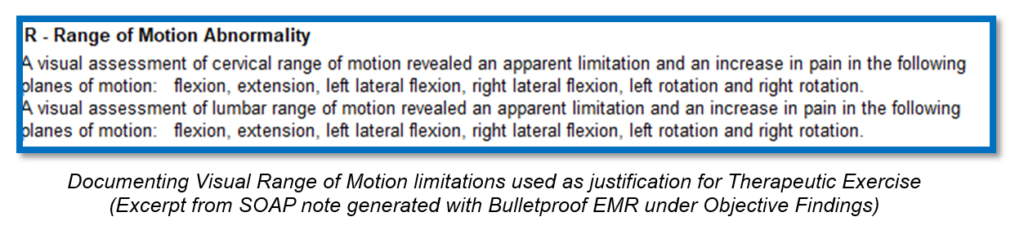
When documenting our Plan, as in what treatment was performed today, it’s important to remember that every form of treatment we provide must be justified by our objective findings. That’s pretty easy when it comes to ice, heat and other passive modalities, like electrical stimulation and ultrasound. Pain and/or muscle spasms are typically enough to justify these modalities. However, the treatments that tend to raise my eyebrows when I review chiropractic records are: Chiropractic Manipulative Therapy Manual Therapy Therapeutic Exercise I’m pretty sure that if I were to ask you what one finding would justify Chiropractic Manipulative Therapy, ALL of you would answer with restriction or subluxation or some other word. Amazingly, though, I’ve been seeing more and more chiropractic records lately in which these are NOT documented. I think there’s an assumption that if you document that you adjusted C3, T4 and L1, it’s obvious that those segments were restricted/subluxated. Don’t assume anything. Let’s start with Chiropractic Manipulative Therapy. If you document in your Plan that C3, T4 and L1 were adjusted, make sure that those segments were noted as restricted/subluxated (other words are OK, too) in your objective findings. The same goes for the extremities. If you adjust the right shoulder, make sure your objective findings reflect a restriction of the right shoulder. So, what about Manual Therapy? This procedure is typically some type of muscle work, so the justification must have something to do with the muscles, such as spasms or trigger points. Stay away from the “paraspinal muscles” when documenting these, though. Be more specific for which muscles, like left trapezius, right levator scapulae, bilateral subscapularis. There’s no requirement to “grade” these spasms or trigger point, so don’t bother wasting your time on that. If you document in your Plan that you performed Myofascial Release, make sure that you name the muscles that were worked on. These same muscles must be noted in your Objective Findings as having spasm or trigger points, though. Make sure you document the amount of time and the reasons why the procedure was performed. How about Therapeutic Exercise? This one has to do with movement, so you’ll want to document which movements/planes of motions the patient was working on, like cervical flexion, cervical left lateral flexion, etc. The justification for this could be as simple as documenting pain in cervical flexion, cervical left lateral flexion, etc. Just like Manual Therapy, make sure you document the amount of time and the reasons why the procedure was performed. Can this be done easily and in very little time? You bet it can. In my EMR, I designed it do this for me. In the Objective Findings part of my SOAP note, I’ll document the spinal and/or extremity restrictions. In the Plan section, I’ll just document spinal/extremity adjustments and my EMR will automatically bring in the specific segments/extremities. When I document the muscle spasms/trigger points in my EMR, I’ll just document Manual Therapy in my Plan and the EMR will automatically bring over the muscles I had already documented in the Objective Findings. When I document pain in various planes of motion in the Objective Findings, I just document Therapeutic Exercises in Plan and the EMR will automatically bring over planes of motion that were previously noted in Objective Findings. Documentation can be easy and exceptional and fast. We just need to know how to justify. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
It is Complicated
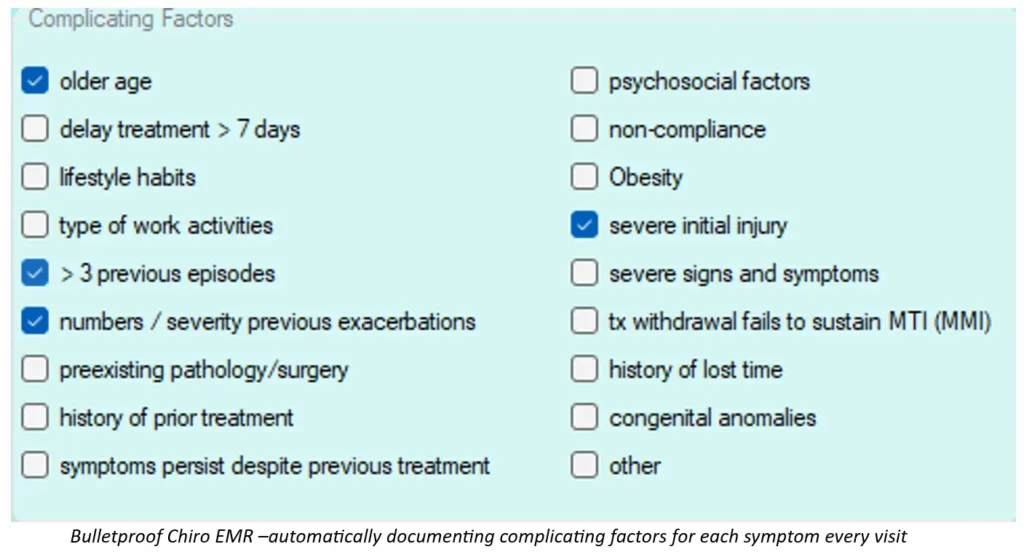
In my previous article, I wrote about how important a great Assessment is in our SOAP notes and how most chiropractors don’t even come close to documenting a good assessment. Some chiropractors complain that some patients respond more slowly than others and that should be taken into consideration. I couldn’t agree more. In fact, a great idea is to document complicating factors for EACH condition you’re treating for each patient, if they exist. A great resource for this is a set of chiropractic guidelines, called Clinical Compass (formerly known as CCGPP). They did all the hard work and found the research to support these. They split up the complicating factors into three categories: Patient Characteristics Injury Characteristics History Patient characteristics include older age, psychosocial factors, delay of treatment > 7 days, non-compliance, lifestyle habits, obesity and type of work activities. Injury characteristics include severe initial injury, > 3 previous episodes, severe signs and symptoms, number/severity of previous exacerbations and treatment withdrawal fails to sustain maximum therapeutic improvement. History includes pre-existing pathology/surgery, history of lost time, history of prior treatment, congenital anomalies and symptoms persist despite previous treatment. I recommend documenting these complicating factors on every visit, just in case your records are ever audited. Medicare, in particular, is notorious for requesting records between “this date” and “that date.” If you don’t have the complicating factors noted on each visit, they may not be present for the dates that are being looked at. And there goes more power out the window. In my EMR, I document any of these complicating factors that exist for each condition on the initial visit. My EMR then has these complicating factors appear on every visit after that – automatically. When documenting the complicating factors in addition to the changing metrics of pain intensity, pain frequency and the outcome assessment scores, your assessment can effectively show how each patient is different and how effective your treatment is, as well as comparing today’s visit to the previous visit. Once we understand and embrace the “rules of engagement,” we can really make our documentation rock. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Pain in the ASSessment
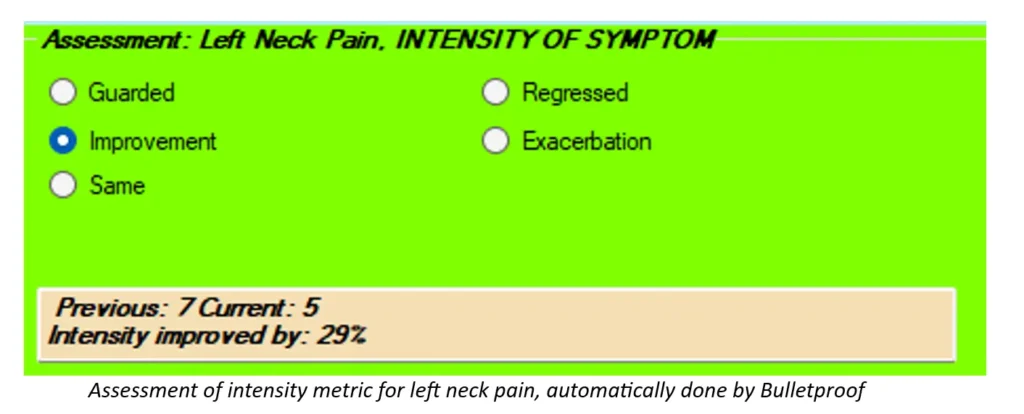
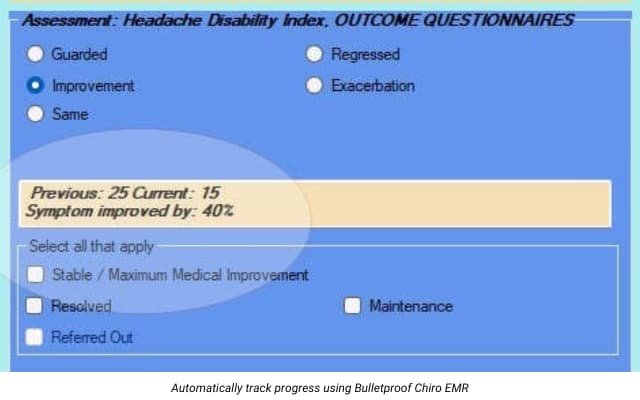
There’s ONE part of our SOAP notes that I’ve been preaching about for years, but it seems as though not many doctors are paying close enough attention to it. It’s the Assessment. Here’s what I see in most records that I review in the Assessment part of the SOAP Note: “Patient is responding well to care.” “Patient is the same.” “Patient is responding slower than expected.” To begin with, according to our friends at Centers for Medicare and Medicaid Services (CMS), we are to document an assessment for each condition that we are treating. If we’re treating a patient for headaches, neck pain and upper back pain, we need to document an assessment for each of these. Even though I’m talking about Medicare, and you may see very few Medicare patients, just remember that Medicare creates the rules that most insurers (and even state boards) follow. If we document well for Medicare, we’re that much closer to the promised land. OK, back to my point. The next thing that Medicare is looking for in the Assessment is how each condition is on today’s visit as compared to the previous visit. That can be problematic. Do they really expect us to look back a visit every time the patient comes in and we have to compare that visit to today’s visit? And what if, on the previous visit, we said something like “Patient presents with neck pain” and on today’s visit we write, “Patient presents with neck pain.” See the problem? Then Medicare wants us to document the effectiveness of our treatment for each condition as compared to the previous visit. Seriously? If you’ve been reading my previous blog posts, you’ll remember that I’m making a big deal about us using certain metrics with our documentation. By using these metrics, we can actually document how each condition is responding since the previous visit AND the effectiveness of our treatment. That’s easy with the right technology. I recently looked at notes from an Administrative Law Judge in a Medicare audit. The particular doctor being audited did a pretty good job of documenting P.A.R.T. and most likely thought he was in the clear. Not so much. The judge noted, for all claims audited, that the doctor failed to document how each condition had changed since the previous visit AND the effectiveness of treatment. Medicare wants their money back – the tune of TENS of THOUSANDS of DOLLARS. If there are any complicating factors, specific to each condition, that may slow the patient’s recovery for that condition, we can document those, too. I make sure that these complicating factors appear on every visit in my SOAP notes. Finally, we can document the diagnoses under Assessment. It really doesn’t matter where in your soap notes you put the diagnoses, but Assessment seems to be the most logical. You’ll want to document both the ICD10 code AND the description, though, not one or the other. Instead of thinking about the Assessment as a pain in the ASSessment, we can think differently about it so we can use it in our favor – by showing the world how awesome chiropractic is and how effective our treatment is – both quantifiably and functionally. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Documenting the Daily Objective Findings
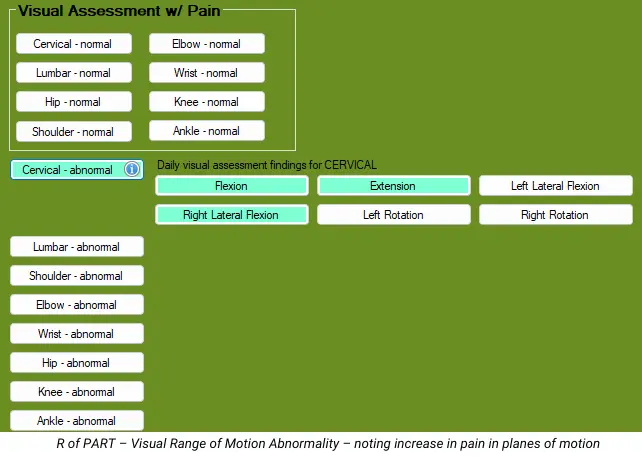
There seems to be some confusion among chiropractors as to what objective findings we need to document on our daily visits. I, and others, have been teaching for a number of years to follow the PART format of documentation for ALL of our patients. This PART format is what is REQUIRED by Medicare, and, to be honest, it works quite well for ALL of our patients. So, let’s review what PART is. The P of PART stands for Pain/Tenderness. As I wrote in a previous article, documenting the metrics of pain intensity and pain frequency will satisfy this component of PART, and it gives us two metrics we can track over time. The A of PART stands for Asymmetry/Misalignment. For this, there are 3 categories: posture, gait and restriction/subluxation. We only are required to document ONE of these, and, if you plan on adjusting your patient, I recommend choosing the restriction/subluxation to document, which makes posture and gait optional. The R of PART stands for Range of Motion Abnormality. No one expects us to actually measure range of motion on every visit – we can save that for the exams. On the daily visits, though, we can simply do a visual assessment of range of motion, noting if there is an increase in pain for each plane of motion or not. Don’t make up fake measurements – there’s no need to do that here. If cervical flexion increases the pain when compared to neutral, it’s positive. That’s it. The T of PART stands for Tissue/Tone Changes. Quit talking about the paraspinal muscles here. Instead, be more specific for the muscles, like left trapezius, right levator scapulae, bilateral supraspinatus, etc. There’s no requirement to grade the spasms or trigger points – just note which muscles are involved. Medicare then tells us that we don’t necessarily have to document all four of these on each visit, but that we HAVE to document at least 2 of the 4, with 1 of the 2 being Asymmetry/Misalignment or Range of Motion Abnormality. To make this easier (hopefully), we need to make sure that everything we do from a treatment perspective must be justified by what you documented as your findings for that visit. For example, if you are doing passive modalities on your patients, like hot packs and electrical muscle stimulation, you’re probably doing that to decrease pain and muscle spasms/trigger points. Make sure that you’ve documented pain and spasms in your notes. If you’re performing manual therapy on a patient, you’re probably doing that to relieve pain and muscle spasms/trigger points. Make sure you’ve documented that. If you’re having your patients perform therapeutic exercises, you’re probably doing that to decrease pain with certain motions and improve function. Make sure you’ve documented that. But here’s one that’s been catching my attention lately in the many record reviews I perform each month. I’m talking about the spinal and/or extremity restrictions/subluxations. Too many of you are documenting the segments you adjusted but are NOT documenting the restrictions/subluxations in your objective findings. You may be thinking it’s implied or assumed, but it’s NOT. As a reviewer, I assume nothing. What you’ve documented is what you’ve documented. If you documented that you adjusted C3, C5, T4 and L1 but you did NOT document that there were restrictions with those segments, I will point out that you did not document a justification for those adjustments. So, here’s how it could look: You perform spinal adjustments and hot packs and electrical muscle stimulation – you need to document the pain (P intensity and frequency), spinal restrictions/subluxations (A) and muscle spasms/trigger points (T). You perform spinal adjustments and manual therapy – you need to document the pain (P), spinal restrictions/subluxations (A) and muscle spasms/trigger points. You perform spinal adjustments and therapeutic exercises – you need to document the pain (P), spinal restrictions/subluxations (A) and increased pain with certain planes of motion (R). You perform spinal adjustments, manual therapy and therapeutic exercises – you need to document the pain (P), spinal restrictions/subluxations (A), increased pain with certain planes of motion (R) and muscle spasms/trigger points (T). That way, every treatment that you perform is justified in your notes. In my EMR, when I document the spinal/extremity restrictions in my objective findings and then click on spinal/extremity adjustments in my treatment plan, the restrictions from my objective findings automatically populate, and the same goes for manual therapy and therapeutic exercise. This is how I blend exceptional documentation with technology to create a great and compliant SOAP note in the least amount of time. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Documentings Musta, Shoulda, Coulda, Part 2

In my last article, I discussed the MUSTs and the SHOULDs of Subjective Documentation, that being Pain Intensity, Pain Frequency and the use of Outcome Questionnaires. Now we’ll tackle the Objective Findings. Even though many chiropractors don’t treat a lot of Medicare patients, please understand that Medicare creates many of the rules. I’ve seen other commercial payors using the Medicare documentation guidelines for their policies, which actually makes it easier for us. Medicare does a great job of narrowing down which objective findings they’re looking for, as part of their PART requirements. The first component of PART is P – Pain and Tenderness, which can fall under the Subjective complaints we discussed in the last article. The next component is A – Asymmetry/Misalignment. Medicare tells us that this includes Posture, Gait and Subluxation/Restriction. Let’s start with the MUSTs. If you plan on performing a chiropractic adjustment/manipulation, you MUST document a reason for it, which would be the subluxation/restriction. This applies to both the spine and extremities. Medicare doesn’t care how we find these subluxations/restrictions, but they do care how we document them. They DON’T want us documenting subluxations/restrictions in regions, such as “cervical, thoracic, lumbar.” They REQUIRE us to document the specific segments, though, such as “C3, T4 and L5.” There is no requirement to document specific spinal listings. They do give another option, though, for when the subluxation/restriction crosses two areas. For example, we can document occiput and C1 or atlanto-occipital. We can document C7 and T1 or cervicodorsal. We can document L5 and S1 or lumbosacral. When I review personal injury records, some chiropractors like to document that they found subluxations/restrictions at literally EVERY level of the spine. That tends to be an “eye roller.” We can be more specific than that. If your treatment centers around posture or gait, and not the subluxations/restrictions, you can document these instead, which makes documentation of the subluxations/restrictions optional, as long as you’re not performing chiropractic adjustments/manipulations. The next component of PART is R – Range of Motion Abnormality. According to the 1997 HCFA/AMA Guidelines for the Musculoskeletal System, all the E/M exam requires is a visual assessment of range of motion noting PAIN, or a palpatory assessment noting crepitation or contracture. For this part of this exam, measured range of motion is NOT required. However, if you want to use range of motion as an outcome assessment to monitor the patient’s progress, you’ll need to measure the range of motion. I don’t mean doing a visual assessment and making up a number – I mean actually measuring the range of motion. Are range of motion measurements a good outcome assessment? Sometimes it is, and sometimes it’s not. If your patient says they feel like they’re not moving well, or if you observe that they’re not moving well, measuring range of motion can be a decent outcome assessment. Make sure when you document this that you mention that you actually measured the range of motion (dual inclinometers for spine, goniometer for extremities) and document what the normal values are (AMA Guides are the most accepted). At re-exams, note the new measurements and if each planed of motion showed improvement, regression or no change, and by how many degrees/percent. Next is the T of PART, which is Tissue/Tone Changes. Don’t document “paraspinal muscles” for this – it’s too vague and tends not to change. Instead, document more specific muscles (i.e. trapezius, levator scapulae, etc.) and if it’s left, right or bilateral. Keep in mind that muscle spasms tend to be more acute in nature, while trigger points can be more chronic. As the patient progresses, make sure you change these to reflect their improvement (or lack of). Do we need to document all four components of PART? Not necessarily, according to Medicare. They require us to document at least 2 of the 4, but 1 of the 2 MUST be A or R. But let’s think of this more practically. If your patient has 1 or more symptoms, document the P of PART with pain intensity and pain frequency for each condition, and an outcome questionnaire for each condition at the first visit and then every 2 weeks. If you plan on adjusting your patient, you MUST document the A (restriction/subluxation) for each segment of the spine/extremity that’s restricted. If you DON’T plan on adjusting the patient, you can document the R. On a typical daily visit with no exam, all you need to do is perform a visual assessment of range of motion noting if there is an increase in pain in each plane of motion. At re-exams, you can measure the range of motion to monitor the patient’s progress. If you plan on performing Therapeutic Exercises with the patient, you’ll want to document the planes of motion that increased pain (R of PART). If you plan on performing Manual Therapy on the patient, you’ll want to document in which muscles you found spasms/trigger points. In other words, you MUST justify ALL of your treatment with your objective findings. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Documentings Musta, Shoulda, Coulda, Part 1
Let’s face it. With regards to our documentation, some doctors don’t say enough, while other doctors say too much. So which is better? Let’s narrow this down to the big three: The Must, the Should and the Could. There are some things we MUST document. They’re required components and if we miss them, we’re toast. Then there are certain things that we SHOULD document. These things aren’t exactly required, but they really enhance our documentation. And then there’s the COULD. There are plenty of things we COULD document, but I’m telling you – most of these are a COMPLETE WASTE OF TIME. Now, if it means a lot to you, ‘cause you just want to say it, well, OK. As long as you know, though, that from a documentation perspective, NO ONE BUT YOU CARES! They aren’t required, they don’t add anything to your documentation and they are just wasting your valuable time. Believe it or not, I want you to document LESS. But the things I want you to document are only the MUSTS and the SHOULDS. Let’s kick the COULDS to the proverbial curb. So what are the MUSTS? Let’s start with what Medicare REQUIRES. I’ve talked about this before: JUST TWO THINGS. And they are…Pain and Function. Everyone wants those same two things. All of the guidelines that are used against us, which we can use FOR us, want these 2 things – for ALL patients. Starting with the Subjective part of SOAP, the first MUST is to document each condition that you’ll be treating. For the purposes of this article, let’s limit it to musculoskeletal. Be specific without going too far. For example, documenting “headache” isn’t enough. We could document “occipital headache.” For neck pain, upper back/middle back/low back pain, we could say “neck/upper back/middle back/low back”, or we can document “neck on the left/upper back on the right/middle back on the left/low back on the right.” Without saying left or right, we’re implying that the pain is not off to one side. The next Subjective Must is the Pain Intensity of each symptom. All of the guidelines want us to have our patients rate their pain, typically from 1-10, with 10 being the worst. The days of documenting simply “neck pain” are over. Here’s an easier way to think of this. Ask the patient, for each condition, if they would call it “mild, moderate or severe.” Most people sort of understand that. Here’s what you need to know: mild is 1-3, moderate is 4-7 and severe is 8-10. If the patient says their pain is MILD, ask them to give you a number between 1 and 3, with 3 being the worst. This tends to make it much easier for the patient to come up with a number. The next Subjective Must is the use of outcome questionnaires. Don’t roll your eyes. This is the easiest, fastest and least expensive outcome assessment we can use. It’s a way that we can effectively track our patients’ progress with regard to their function. Better yet, ALL of the various guidelines want this. It’s also required by Medicare. There are valid and reliable outcome questionnaires for practically every musculoskeletal body part. All we need to do is give the patient ONE questionnaire for each condition that we’re treating. Some of you have been using the Revised Oswestry for low back pain and the Neck Disability Index for neck pain, both which are fine. I prefer the Neck Bournemouth Questionnaire and the Back Bournemouth Questionnaire, since these are only 7 questions each, meaning they’re faster and easier for patients to complete, and they also have a psychosocial question, which is missing from Oswestry and NDI. There’s a great headache questionnaire and several questionnaires for the upper and lower extremities. At the very minimum, we should have the ACTIVE patient complete the questionnaires on the FIRST visit and then “every 30 days or sooner”, which is what Medicare requires. Now let’s talk about the Subjective SHOULD. The first SHOULD is Pain Frequency. I talked about this in my last article. While not required, it can add SO MUCH to our documentation, especially if the pain intensity isn’t changing very quickly. The best way to document this FREQUENCY is with an actual percentage of awake time. Stick to 5 or 10% increments, like 50%, 75%, 100% and so on. Your documentation is MUCH better if the intensity is stuck at a 6/10 for 5 visits, but the frequency goes from 100%, to 95%, to 85%, to 80%, to 75%. This is also MUCH better than saying “occasional, intermittent, frequent and constant.” While they’re better than not saying anything, they still suck because your patient can be stuck in the constant range for 2 months and your documentation looks like they’re not getting any better. The next Subjective SHOULD is how often we have the patient complete the outcome questionnaires. I mentioned above that Medicare requires that we have the patients complete these “every 30 days of sooner.” However, I recommend that we do these questionnaires EVERY 2 WEEKS, so we can see and track the patient’s progress. Another reason for the every 2 week re-assessment is that several of the guidelines say “if the patient does not show signs of objective improvement in any two successive two week period, referral is indicated.” I know, these outcome questionnaires are subjective and not objective, but that’s not what they mean. They just want to see measurable and functional improvement. If there’s no measurable and functional improvement after 2 weeks, you can change something about your treatment and go for another 2 week trial of care. As long as you’re showing improvement, you’re good. As long as you’re showing that you’re changing the treatment after no improvement, you’re good – at least for another 2 weeks. These Subjective MUSTS and SHOULDS let us document in terms of METRICS. Tracking these numbers will enable us to show how each metric is changing over time with our treatment. It will also enable us to document specific treatment goals which will make our documentation exceptional. But…have you ever had the experience when the patient tells you something that can’t quite fit into a metric? For example, I heard this the other day: “My pain went to a 0 after my last visit, and it lasted for
Documenting Subjective Complaints
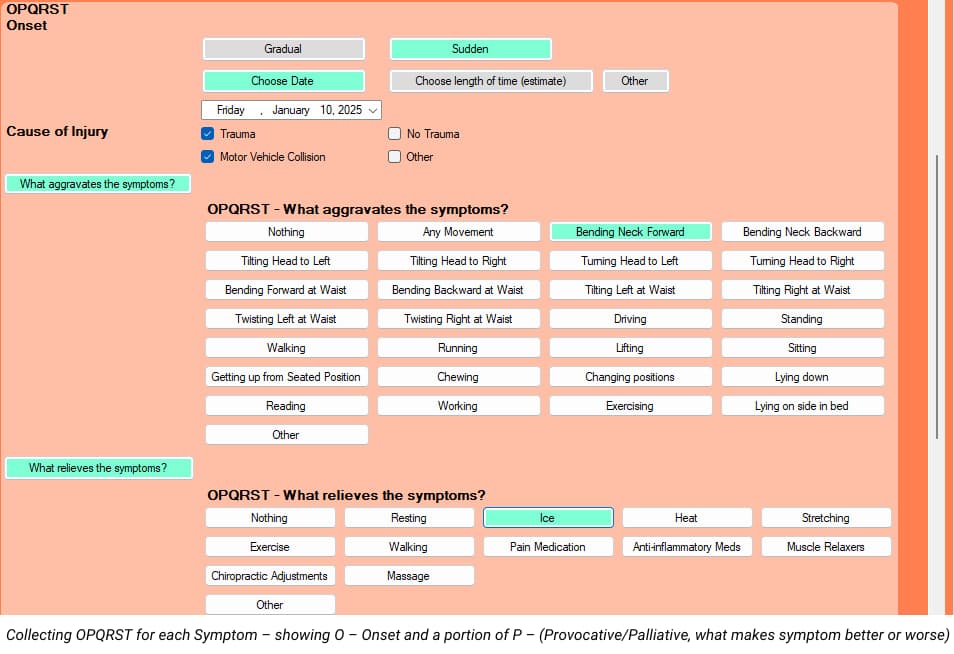
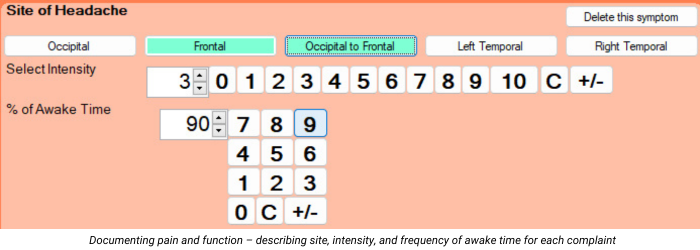
After being in practice for 32 years, teaching documentation and coding for about 20 years, reviewing records and performing IMEs for a lot of years, I see and hear the same things over and over again with regards to documenting subjective complaints. Let’s make this easy. Initial Visit According to the Mayo Clinic, 80% of the proper diagnosis comes from a good history. Unfortunately, many chiropractors tend to take shortcuts on the history, perhaps in the interest of saving time. The standard of history taking has been the OPQRST for many years. There are a few variations of this, but they all tend to get the same information. Before you think of not asking and documenting all of OPQRST, think about which of these items are less important than others. I teach doctors to document ALL of OPQRST on the first visit for ALL new patients, but there’s an easy and fast way to do it. Once we get that information at the beginning of a case, we don’t have to document all of that on subsequent visits. So, let’s review the OPQRST: Onset – when the patient presents with multiple conditions for which you will treat, you need to document OPQRST for EACH complaint, not just the CHIEF complaint. You’ll want to document how each condition started (trauma vs. no trauma), when each condition started (specific date or time frame) and if each symptom began suddenly or gradually. Provocative/Palliative – document both provocative and palliative for EACH condition you’ll be treating. In other words, what makes the neck pain better and worse, what makes the low back pain better and worse, etc. Quality – describe the quality of EACH symptom you’ll be treating. Radiate – document if each condition is radicular or not. If a symptom is radicular, use the language of Anatomical Position so anyone seeing your records will know what you’re talking about. For example, in the language of Anatomical Position, “arm” refers to above the elbow and “forearm” refers to below the elbow. “Thigh” refers to above the knee and “leg” refers to below the knee. You can be specific by documenting the neck pain radiates to the right posterolateral arm, right posterolateral forearm and to the first 2 digits of the right hand. Site/Severity – Be specific without going overboard. Instead of documenting “headaches”, we can document “occipital headaches.” For neck and back pain, we can document if it’s the whole neck or back or left or right. For severity, more and more payers and even reviewers like me want to see a 0-10 pain scale (10 being the worst pain imaginable) for each complaint. To make this easier for my patients, I start by asking them if they would call their pain, for each symptom, Mild, Moderate or Severe. If they say Mild, I explain that’s between a 1 and a 3 and ask them for a number. For Moderate, that’s between a 4 and a 7, and for severe, that’s between an 8 and a 10. That tends to make it easier for them to come up with a more accurate number. So, ask verbally for mild, moderate or severe for each symptom, but only to get them to an actual number that you’ll document. Timing – On the first visit only, document, for each symptom that you’re treating, if the pain is worse at a particular time or times of the day (morning, afternoon, evening, night), or if the symptom is unaffected by time of day. For all visits, document what percentage of their awake time they notice each symptom. BEWARE of using the ranges of Occasional, Intermittent, Frequent and Constant, though. These ranges are defined as: Occasional: 0-25% of awake time Intermittent: 26-50% of awake time Frequent: 51-75% of awake time Constant: 76-100% of awake time The problem with these ranges is that they’re too broad (25 points). Your patient’s symptom could appear stuck in a particular category for MONTHS, which can make your documentation weaker by showing no change. Instead, I recommend document an actual percentage of time that each symptom is noticed (5 or 10 percent increments, though-don’t get carried away by documenting “23% of the time.” If you document on one visit that the frequency of the symptom was 100%, but on the next visit it reduced to 95%, even though just a slight change, it’s still shows some improvement. It’s much better to show the frequency went from 100% to 95% to 90% to 85% to 80% to 75% than to show constant, constant, constant, etc. Gregg’s Tip: I designed my intake paperwork to capture all of this information, so my patients do all of the heavy lifting for me. We send them the paperwork via e-mail and instruct them to bring the completed forms with them to their appointment. I also designed my EMR to be the same flow and direction of my paperwork, which makes it MUCH easier for the doctor or staff to input the information. Once we get all of that information entered on the first visit, all subsequent visits are QUICK AND EASY – I just change the metrics of the Severity and Frequency of each symptom. The next part of documenting subjective complaints is to establish a “measurable baseline of function” for each complaint. A great, easy, fast and inexpensive way to do this is with valid and reliable outcome questionnaires. Medicare requires this, many commercial insurers require this and for workers comp and PI, us reviewers are looking for this. You want to document the scores on the outcome questionnaires on the very first visit, which can then be used as a treatment goal. While Medicare requires that we perform these functional outcome assessments at a MINIMUM of every 30 days, I recommend performing these outcome questionnaires every two weeks for the active patient and once or twice per year for maintenance patients. If all chiropractors would do these outcome questionnaires every 2 weeks for ALL active patients, our documentation would be tremendously improved overnight. Gregg Friedman, DC,
Just Two Things
I remember the “good ‘ole days” of chiropractic. The days when it seemed that everyone in America had health insurance, when the typical deductible was about 100 bucks and the patient only had to pay 20% of the charges. And their policy limited chiropractic treatment to only “UNLIMITED VISITS.” Sigh… When a new patient came in, we did the ortho/neuro exam we all learned in chiropractic school, found a few areas of pain, some radicular signs every now and then and recommended a treatment plan. Patients seemed happy to start, excited it was affordable (since their insurance paid for the bulk of treatment). They started feeling better quickly and referred their friends and family in. And let’s not forget our favorite Medicare patients! Once they felt better, many of them wanted to continue to come in for maintenance. Yep, we just kept on billing Medicare…for years. For the personal injury patients, we’d examine, treat and bill, for pretty much as long as we wanted or until we got bored. No one ever challenged us. We’d send our bill in, and it got paid. All of it. Every penny. And no one ever asked to see our documentation. Ahhh…the good ‘ole days. That was about 30 years ago. I guess you can say it’s changed a bit since then. These days, patients may have health insurance, but their deductible is often higher than $5000 per year and co-pays are often more than our cash fee for an adjustment. Medicare is mad at us. Personal Injury is mad at us. Workers Comp, in many states, won’t even talk to us. Chiropractic offices are opening up all over the country, charging about $15 for an adjustment. Yeah, that helps. We were taught in chiropractic school and by every consultant on the planet to perform periodic re-exams on each patient. We’d find that the orthopedic tests caused a little less pain, palpation seemed to cause a little less tenderness and range of motion seemed to be getting better, as far we could tell. More and more, chiropractors are being asked to send our records to the insurance company so they can see if our treatment is appropriate. How rude. So, we send in a copy of our travel card, or even better, our fancy type-written notes from some EMR or EHR that we spent way too much money on or took more time to document than it did to adjust the patient. We send in our exam forms that show the patient is feeling less pain, less tenderness and seems to be moving better. And then we get told that our care was not “medically necessary” and no more treatment is appropriate. What in the world are they talking about? I know many doctors reading this are nodding their head in agreement. I got upset over the way I felt I was being treated, so I made it my mission to find out what the heck they were talking about. Apparently, someone changed the rules of documentation and no one bothered to tell us about it. So, what did I discover? The health care industry (doctors, insurance people, even attorneys) love tests. More specifically, tests with numbers. Think about it – blood tests have numbers. Urinalysis tests have numbers. All kinds of tests have numbers. What does a typical report of findings sound like from a medical doctor? Think about it. “Well, Mrs. Smith, we had some blood work done for you, and this is what we found. This is normal. This is you.” The patient nods. The doctor explains what it means and recommends some medication that the patient should take three times per day for the next 6 weeks. The patient nods. The doctor continues that, in six weeks, we’ll re-do the blood tests and see if the patient is normal or, at least, on the right track or not. The patient nods. Hopefully, as the tests become normal, the patient feels better, too. There was no selling involved. Just a doctor being, well, a doctor. So what are we chiropractors supposed to do? I mean, it would be AWESOME if we had a blood test that shows that the patients have subluxations here, here and there. It would be FANTASTIC if we could test their blood again after we’ve treated them for a period of time and see that their subluxations are improving here, here and there. Maybe one day we’ll have those kinds of tests, but for now… We don’t need them. The health care world basically wants two things from chiropractors. They want us to show that we have relieved the patient’s pain and improved their function. That’s it. Pain and function. Medicare now requires ALL doctors to report certain measurements to them to show that the treatment is being effective. Luckily for chiropractors, they currently only require TWO things. That’s right – Pain and Function. As a reviewer for many personal injury cases, I can tell you we look for the same two things – Pain and Function. What do the Workers Comp carriers want? Yep – pain and function. Think about your cash paying patients. Sure, they love it that they’re feeling better, but don’t you get excited for them when they say that they were able to play on the floor with their kids for 10 minutes longer than they could before? Or they’re driving a golf ball 30 yards farther than they did a month ago? Pain and function. That’s what the health care universe is looking for. Medicare takes it even a step further. They actually state in their documentation guidelines for chiropractors what they want. Unfortunately, this may be one of the best kept secrets in our profession. Medicare actually states that they want us to have the patient complete outcome questionnaires. That means, instead of asking individual questions like “How long can you sit before your butt goes numb?” or “How long can you read before your head feels like it’s
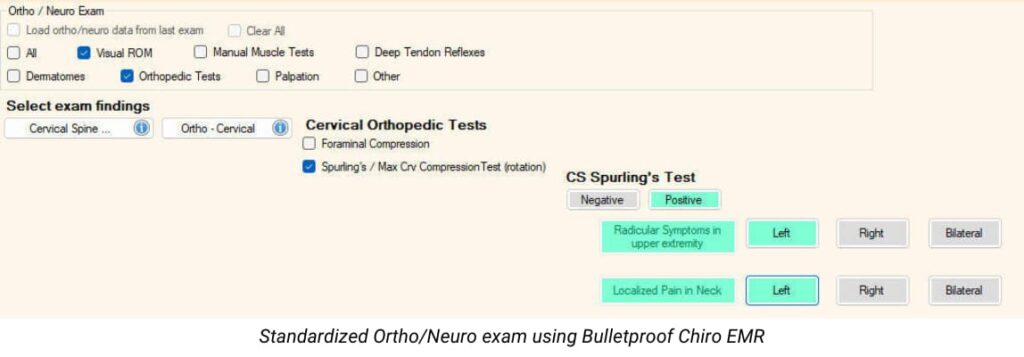
A Failure to Communicate
In the old movie, Cool Hand Luke, the Captain said to Luke, “What we’ve got here is failure to communicate.” This has been a major problem with the chiropractic profession since our inception. So many people who’ve never been to a chiropractor have simply no idea what it is that we do and why we do it. In fact, the rest of what I like to refer to as the “Health Care Universe”, which includes other health care providers and payers, has very little understanding of what we do or why we do it. Why not? It’s because of our documentation. How do I put this gently? You see, as a profession, our documentation, um, sucks. I’m a 2nd generation chiropractor and I’ve been treating patients for more than 31 years. I’ve also been reviewing LOTS of records and performing IMEs for quite awhile. If you could see what I see…you might have a better understanding of what I’m talking about. We seem to have little to no standardization of how to perform a history and exam. One patient can go to 10 different chiropractors, and that one patient will likely get 10 different exams, all kinds of different diagnoses and 10 completely different treatment recommendations – some for 2 visits, some for 6 visits and some for a pre-paid package of 53 visits. We’re all over the place, and it makes us, as a profession, look ridiculous. Many chiropractors ask me if they should be sending their patients’ primary care doctor their notes. My answer is always…”NOT IF THEY SUCK.” But, if you document properly, using the “universal” language of healthcare, not language that only chiropractors understand, then, by all means, send the notes. Many chiropractors tend to have a love/hate relationship – hmmm, check that – a hate/despise relationship – with Medicare. What has been our biggest problem with Medicare over the years? Yep – our documentation. Personal Injury? Yeah, the documentation. Blue Cross Blue Shield and other payers? More and more of them are producing guidelines that are putting chiropractors into a full blown panic attack. Why do they keep doing this to us? I suspect it’s because we, as a profession, have done such a poor job of documenting what it is that we do and why we do it. At least that’s a big part of it. So how do we fix it? I can just say “document better,” but that’s too ambiguous. We need to standardize our exams more. We need to address BOTH pain and function, not just pain. Let’s start with the History. Too many chiropractors are taking shortcuts on the history. The standard in the Health Care Universe is the OPQRST method, but we’ve got to ask and document ALL of those letters, and we need to document them for EACH condition that we’ll be treating. We need to understand what the ortho/neuro exam is actually for, and what it’s NOT for. We need to understand how to document the findings of the exam. If I see one more time a chiropractor’s records for a non-radicular patient in which the chiropractor notes Grade 2 muscle weakness, I’m going to spit. We need to wrap our head around using outcome assessments for ALL of our patients. This is not a Medicare thing or a PI thing – it’s a DOCTOR thing. But we need to figure out which outcome assessments are more powerful, take less time and are most cost-effective. We need to accept and embrace some guidelines (I know, a four-letter word, so to speak) that actually HELP us help our patients. The CCGPP Guidelines are an EXCELLENT place to start. We need to know exactly WHEN to re-assess the patient and HOW to determine if our treatment has been effective or not and if we’re justified to continue treating the patient – or not. We need to know exactly when ACTIVE care ends and MAINTENANCE care begins. And, here’s the big one – we need to be able to do ALL of this in the LEAST amount of time, with the LEAST amount of effort (documentation, not the exam or treatment) and, yes, the LEAST amount of cost. Is all of this even possible? You bet it is. But only if we stop failing to communicate. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
