Let’s Have More Fun-ction

More about… Medicare, Medicare, Medicare. In my last article, I wrote about the TWO THINGS that Medicare wants from us. The first thing is PAIN. So now, let’s discuss the SECOND thing Medicare wants from us. Function Medicare requires that we perform a Functional Outcome Assessment for our patients. They define a Functional Outcome Assessment as “patient completed questionnaires designed to measure a patient’s limitations in performing the usual human tasks of living and to directly quantify functional and behavioral symptoms.” But… They also state that we must use a “standardized tool” and document a care plan “based on the identified functional outcome deficiencies.” And… They continue…“Documentation of a current functional outcome assessment must include identification of the standardized tool used.” So what is a “standardized tool?” According to Medicare, it’s “a tool that has been normalized and validated.” That means you can’t just make one up. But there’s more… Medicare also states that “A functional outcome assessment is multi-dimensional and quantifies pain and neuromusculoskeletal capacity; therefore the use of a standardized tool assessing pain alone, such as the visual analog scale (VAS), does not meet the criteria of a functional outcome assessment standardized tool.” So how often do we need to have our patients do these? Medicare states, “The intent of this measure is for a functional outcome assessment tool to be utilized at a minimum of every 30 days.” But there’s more… Here’s Medicare’s rationale: “Standardized outcome assessments, questionnaires or tools are a vital part of evidence-based practice. Despite the recognition of the importance of outcomes assessments, questionnaires and tools, recent evidence suggests their use in clinical practice is limited. Selecting the most appropriate outcomes assessment, questionnaire or tool enhances clinical practice by (1) identifying and quantifying body function and structure limitations; (2) formulating the evaluation, diagnosis, and prognosis; (3) informing the plan of care; and (4) helping to evaluate the success of physical therapy interventions (Potter et al., 2011).” Medicare also tells us that “clinicians should use validated self-report questionnaires/tools that are useful for identifying a patient’s baseline status relative to pain, function, and disability and for monitoring a change in a patient’s status throughout the course of treatment.” Remember what I told you in my last article, though. Medicare drives this whole train. Everyone else follows Medicare. They created the documentation guidelines. They guide the CPT and ICD10 codes. So, instead of fighting them (and losing), we need to understand their perspective and follow their rules. So, let’s break this down. For ALL of our patients, regardless if they’re a Medicare patient, cash-paying patient, personal injury patient or anyone else – it’s time we standardize this ONE thing – our documentation. Document the pain intensity and pain frequency for each complaint on every visit. Have the patients complete a functional outcome assessment utilizing a standardized tool. Document the name of each functional outcome questionnaire and its score. Formulate a treatment plan based on the functional outcome assessment score. And don’t panic. This can be done in very little time. The results are worth it. Be BulletProof.
What a Pain

Medicare, Medicare, Medicare. I know, we’ve had this hate-hate relationship with them for so many years. So many chiropractors are afraid of it and hate the reimbursement. I get it. But… You need to understand that Medicare drives this whole train. Everyone else follows Medicare. They created the documentation guidelines. They guide the CPT and ICD10 codes. So, instead of fighting them (and losing), how ‘bout we understand their perspective a bit more. Medicare wants TWO things from us. The first thing is PAIN. In 2009, the American Pain Foundation identified the following pertinent facts related to the impact of pain: 76.5 million Americans suffering from pain. Pain affects more Americans than diabetes, heart disease and cancer combined. It is the number one reason people seek medical care. Uncontrolled pain is a leading cause of disability and diminishes quality of life for patient, survivors, and their loved ones. It interferes with all aspects of daily activity, including sleep, work, social and sexual relations. Under-treated pain drives up costs – estimated at $100 billion annually in healthcare expenses, lost income, and lost productivity – extending length of hospital stays, as well as increasing emergency room trips and unplanned clinic visits. Medically underserved populations endure a disproportionate pain burden in all health care settings. Disparities exist among racial and ethnic minorities in pain perception, assessment, and treatment for all types of pain, whether chronic or acute. Stewart et al. (2003) identified almost thirteen percent of the total workforce experienced a loss in productive time during a two-week period due to a common pain condition: 5.4% for headache; 3.2% for back pain; 2.0% for arthritis pain; 2.0% for other musculoskeletal pain. What does Medicare want from us with regard to documenting PAIN? They simply want us to document a pain assessment using a standardized tool(s) on each visit AND documentation of a follow-up plan when pain is present. There are a number of standardized tools that Medicare gives as examples, but the easiest and fastest is the Verbal Numeric Rating Scale. This is the familiar 0-10 scale, with 10 being the worst pain imaginable. Add to that the % of time the patient notices that condition, and you’ve got Pain Assessment locked up. Be BulletProof.
The What and The Why
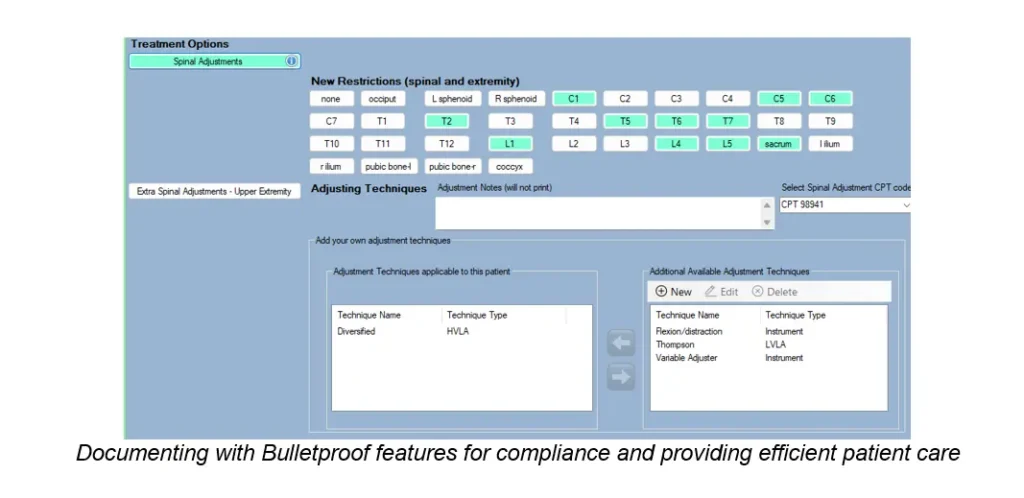
When we think of documenting a SOAP note, we need to be sure that we connect all the dots. One of the biggest problems I see in the many chiropractic records I review is that the treatment is not justified by the findings. And it’s easily corrected. If you perform an adjustment/CMT at C3, what is the justification for that? The simple answer is restriction/fixation/subluxation at C3. If you perform an adjustment/CMT to the right shoulder, the justification would be restriction/fixation/subluxation of the right shoulder. You also want to be sure there is asymptomatic complaint and diagnosis that corresponds to the finding. Think of it this way: symptom + finding + diagnosis = justification for treatment. Manual Therapy (97140) Manual Therapy is another one that comes up frequently. CPT tells us that manual therapy (97140) is performed in order to increase functional performance, increase range of motion, decrease inflammation and reduce muscle spasm. That tells us that our objective findings should mention some type of decrease in functional performance, decrease in range of motion, increase in inflammation or the presence of muscle spasms. Therapeutic Exercise (97110) CPT tells us that therapeutic exercises are performed in order to develop strength and endurance, range of motion and flexibility. The justification that we should document for this should mention some type of abnormality of strength and endurance, range of motion or flexibility. When we document properly and understand that the Why supports the What, we’re one step closer to being… BulletProof.
How to Document for Wellness Patients

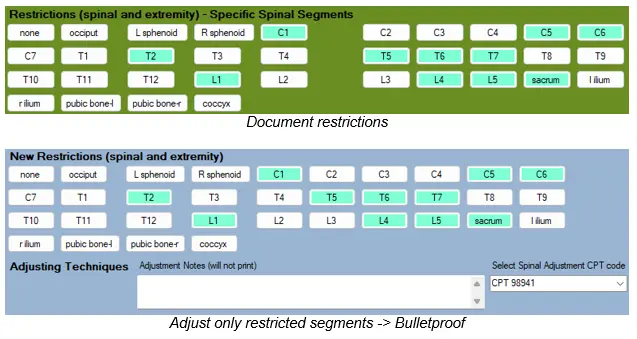
This question comes up periodically. “What do we need to document for our maintenance patients?” Let’s first define what we mean by “maintenance” patients. Some of these patients come in with no symptoms – they just like to get adjusted periodically. Other patients, though, have some level of chronic pain or discomfort that never seems to go anywhere – it just stays the same all the time and they find that getting chiropractic care keeps it from getting worse. The type of care these patients get is called “supportive care.” For the asymptomatic maintenance patients, we still need to document a SOAP note for them. Here’s what I recommend: 1. For Subjective Complaints, you can simply document “Patient X is here today with no symptoms, for the purpose of a maintenance adjustment.” 2. For Objective Findings, if you plan on adjusting them, document the restrictions/subluxations, but at specific levels, like C3, T4 and so on. If there are any muscle spasms or trigger points, make sure you document them. 3. For Assessment, there are no metrics to consider, so there’s no need to compare to the prior visit. However, you should still document the diagnoses, both code and description. 4. For Plan, document what you did. If you adjusted the patient, make sure you document the specific segments adjusted. For patients receiving “supportive care,” you should still document the metrics of pain intensity and pain frequency, even if they don’t change much. Document your daily findings (Asymmetry/Misalignment, Range of Motion Abnormality, Tissue/Tone Changes). If you are adjusting the patient, definitely document the spinal/extremity restrictions (asymmetry/misalignment). If you perform any other treatment, make sure each procedure is properly justified in your SOAP notes. Document the Assessment, which should include complicating factors and diagnoses. Does anyone actually PAY for supportive care anymore? Every now and then, but not too often. Workers Comp has paid for supportive care in the past, but they’re starting to move away from it. This is something the patients should pay for out of their own pocket. Be BulletProof.
Documentation, The BIGGER Picture
Doctors ask me all the time why I chose the worst subject in the history of subjects to teach – documentation. Originally, it was simply because many of us were getting absolutely hammered by insurance companies (commercial and auto) and our reimbursement was getting hit hard, or we were asked to PAY BACK money that had been paid to us (think Medicare and PI post-payment audits). Back then, I spent a lot of time, energy and money to figure out what the hell these insurers were talking about how we can finally beat them at their own game. But, then, something happened. I started to get requests from these same insurers to review chiropractic records. The first few I saw, I thought, “Wow. These are pretty bad. Good thing this is just a small sample size.” After reviewing a few hundred more, I thought… Ruh Roh. I mean, let’s face it. None of us really like to or even WANT to document. We know we have to (sort of…most of us), but we don’t want to do it. Trust me – I get it. But in my 33 years as a chiropractor and growing up with a father who was a chiropractor (60 years – can you believe that?), I’ve thought and heard from other chiropractors how no one takes us seriously, how we can never seem to get ahead legally and how that old friend “cultural authority” has seemed to elude us for all these years. But it wasn’t until I started looking at chiropractic records – and I mean, a LOT of them – that I realized that much of it is… Our Fault. Now, don’t get me wrong. I really believe that what we do as chiropractors is still as mind-blowing now as it was when I started practicing all those years ago. I really believe that the VAST majority of chiropractors mean well and just want to do their best for their patients. But the way we communicate what we do – what the rest of the world SEES from us – in our documentation – is not just bad – it’s downright AWFUL. And don’t think I’m giving you crap because you might be using a travel card and haven’t spent thousands of dollars on some computerized software (most of which suck, by the way) – I’m not. I’m giving an equal amount of crap to the doctors who think that because they DID spend a lot of money on software, that makes them special and their documentation better. Nope. They’re just wrong. Then I hear other people teaching that our documentation should “tell the story.” As one who gets to read this crap all the time, let me save you some trouble. We’re not reading your damned story. Not now, not ever. But there ARE certain and specific things we ARE reading. Some doctors document hardly anything. That’s a problem – maybe. Other doctors are just throwing as much crap as they can into their documentation with the hope that some of it sticks. I hope they didn’t spend too much on THAT software. So what is that that I’m looking for in your documentation? What ONE thing am I looking for on your FIRST visit that will help you TREMENDOUSLY with your future care? I’ll tell you… Next Time.
The Numbers Game
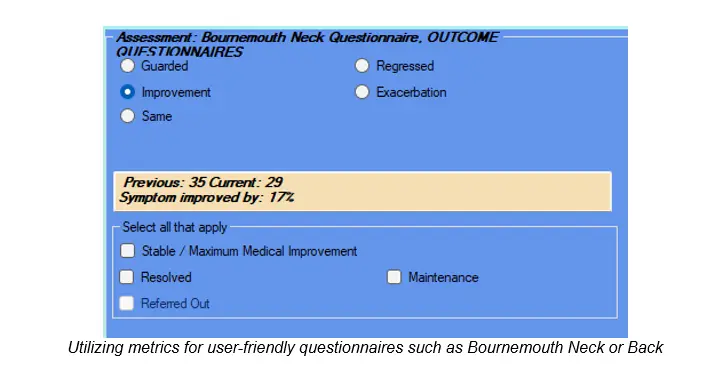
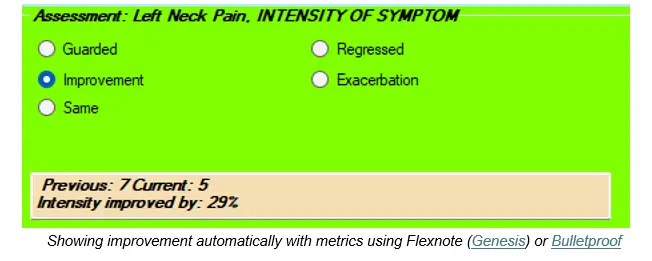
Even though Chiropractic has been around since 1895, it’s still a pretty young profession, in the grand scheme of things. While the rest of healthcare has embraced the use of numbers for years, chiropractic is still pondering the idea. While numbers aren’t the “end all,” if used properly, they can be of enormous benefit to chiropractors and our patients. When you go to a medical doctor, the visit often includes certain metrics of which they like to keep track: height, weight, blood pressure, temperature, pulse, respiration. Medical doctors often perform blood tests and a urinalysis on their patients, too, which helps them arrive at a diagnosis and enables them to track the metrics to see if the patient is improving or not with treatment. Even dentists use metrics. I was fascinated a few years ago when a visited a dentist friend of mine for a deep cleaning. His hygienist actually measured my gums and they were able to determine where I needed work and where I didn’t. So what about us? For all these years, chiropractors have relied on our patients telling other people how much better they feel with chiropractic. But… Numbers can make it even better. It’s one thing to affirm that the patient is feeling better. It’s another thing, though, to tell them that the intensity of their pain has improved by 18% and the frequency of their pain has improved by 24% since their previous visit. Chiropractors have been saying for years that we improve people’s function. We can take it even further by actually SHOWING our patients how MUCH we’ve helped them improve their function. The easiest and fastest way to do this is with outcome questionnaires. I saw you roll your eyes at me. We’ve got to make this easier than it is now, though. Some of you have been giving your patients the Neck Disability Index and Revised Oswestry Low Back Pain Disability Index. Let’s face it – your patients hate them and YOU hate them. I haven’t used either of those questionnaires in about 20 years. I switched to the Bournemouth Neck Questionnaire and the Bournemouth Back Questionnaire. Why do I use these? They’re only 7 questions each, which is 30% shorter and faster than the NDI and Oswestry, and they tend to be much easier and faster for patients to complete. There’s a great headache questionnaire that I use that can track how much functional improvement my patients achieve with treatment. There are outcome questionnaires for practically every musculoskeletal body part. Without overloading our patients with questionnaires, we can use the appropriate ones at the appropriate times and you’ll be amazed at how we can show how effective our treatment has been. When I show my patients the actual quantitative and functional improvement, they get EXCITED! If you want to get more referrals from medical doctors, we need to speak their language, which revolves around…NUMBERS. If you want to solve the “medical necessity” argument for Medicare and other insurers, document METRICS. If you want to show the world how effective chiropractic is at relieving pain and improving function, document METRICS. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
It’s Not About Insurance
I know, good documentation helps us get reimbursed better by insurance. I get it. But… It’s Not Just About Insurance. I graduated chiropractic college in the late 1980s. Back then, no one cared about our documentation. Ever. We would scribble meaningless stuff on ridiculous travel cards, but it worked for us back then. No one ever looked. Not even for PI. Then, one day, it changed. The health care world wanted more from us. The problem was, it took them YEARS to tell us what they really wanted. I want you to think about documentation differently. Instead of thinking of it like the worst and most time-consuming part of practice, let’s start thinking of our documentation as … How we communicate who we are and what we do to the rest of the world. Right now, the rest of the health care universe just doesn’t quite understand us or know what to do with us. We keep telling them how effective chiropractic care is and how cost effective it is, but we’re not communicating that very well. We’re just not speaking in their language. This is why exceptional documentation, in which we document certain metrics at the right time and in the right way, can finally show the world who we are. Many of us, over the years, feel uncomfortable with a report of findings. It often feels like a sales pitch. What if we can explain to the patient what is going on with the two most important things to them: pain and function? By documenting and calculating metric improvements in both, we can easily tell the patient what normal/ideal is and what they are. Then we can simply ask them what they want to do about it. We can tell them how much measurable improvement they’ve achieved and if there is more measurable improvement to be had. All based on metrics. No sales pitch. No charisma needed. Just numbers that are relevant to the patient. But I’m a chiropractor, too, and I know how many of us think. I’m the same way. First, this all sounds well and good, but if I can’t do it really quickly, I’m hesitant to change. Second, it’s got to be easy. Is this doable without technology? Of course, it is. But it’s going to take more time than you probably want to spend. Is this doable with technology? Of course, it is. But almost all software programs don’t do it. I do it. Every day. With every patient. And, for most visits, it takes me SECONDS. It doesn’t matter if it’s for a cash paying patient, a Medicare patient, an insurance patient or even a workers comp or PI patient. That should be irrelevant. Same exceptional documentation for all patients. It’s not just about insurance. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
The Shift

Major League Baseball has been analyzing data, called Sabermetrics, since the middle of the 20th Century. All year long, even in the off-season, baseball people are looking at data in order to determine a variety of scenarios that will help them get the best outcomes (wins). It’s gotten so crazy that there’s now a strategy called a “shift,” in which some of the infielders and outfielders shift more toward one side of the field because the data tells them that the hitter hits the ball to that side of the field a certain percentage of the time. In healthcare, there’s been a “shift” toward evidence-based healthcare. According to Official Disability Guidelines (ODG), the problem with evidence-based medicine (EBM) is that there is not enough of it. According to an Executive Summary from ODG, “randomized, double-blind, placebo-control clinical trials (RCTs), and meta-analysis of those trials are costly and time-consuming. They do not exist for many routine, low-cost interventions with little incentive to perform the study.” How does this apply to chiropractic? Rather than thinking about “evidence-based” chiropractic, let’s consider “outcomes-based” chiropractic. In fact, the entire healthcare system has begun a massive transition towards value-based care, in which health care systems will be rewarded not by how much treatment they provide, but how well it works. The beauty of this is…chiropractic works great. We just need to SHOW it works great. Don’t think of “outcomes-based” chiropractic as just an insurance thing, although it’s what ALL of the payors want. Instead, think of it as a way that we can finally SHOW the world how effective our treatment really is. We can accomplish this EASILY, by documenting certain metrics with regards to our patient care. For which metrics do we need focus? Believe it or not, Medicare answers that for us. They require that we keep track of just TWO things: Pain and Function. All of the payors want to see improvement in Pain and Function. Even our patients want to experience improvement in Pain and Function. We’re already doing it. Now let’s document it. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Sometimes Less is More – A Short Story
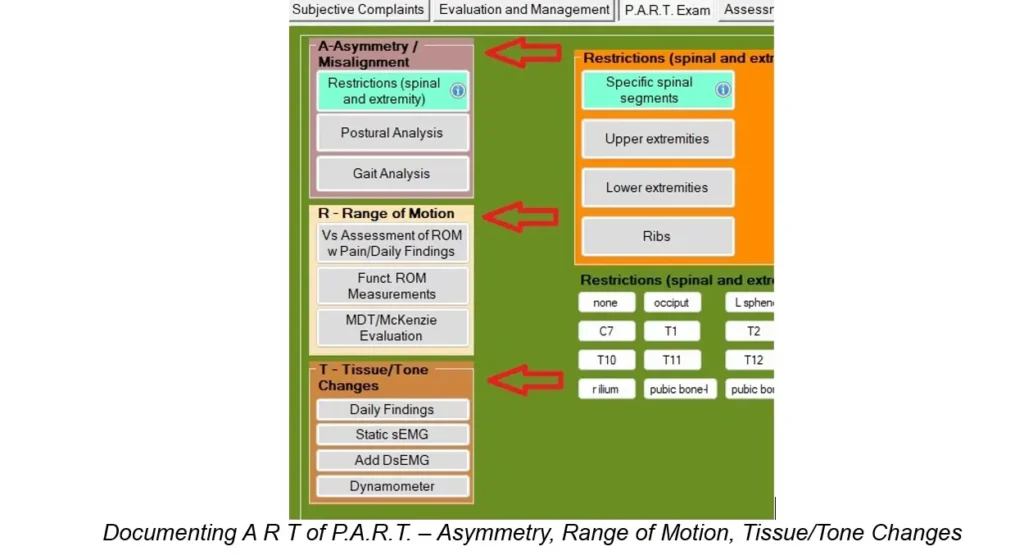
Documentation is a funny thing. For years, chiropractors have been told that our documentation has to “tell the story.” Unfortunately, many chiropractors take that to think they have to write a novel for each patient encounter. The good news is… You may be talking too much. I agree with the premise that we need to tell the story about what is going on with our patients and with each patient encounter. As one who reviews a lot of chiropractic records for insurance companies and attorneys, I can tell you that saying too much does not help. We need to know what parts of the story need to be told. Let’s take our SOAP notes. For the Subjective part, it’s important to document a thorough history on the first visit. The standard for many years has been the OPQRST (onset, provocative/palliative, quality, radiating, site/severity and timing) format, which is required by Medicare. We need to document all of these letters for EACH condition we’ll be treating. On this initial visit, we also need to establish measurable and functional baselines. The key which will make this easier and faster is the use of metrics. Instead of saying “neck pain,” or “moderate neck pain,” we could have the patient rate the intensity of each symptom with the Verbal Numeric Rating Scale (0-10). For more accuracy, we can also have the patient tell us the percentage of their awake time they experience each symptom. Using 5 or 10% increments of time is all we need and is much better than documenting very broad ranges like Occasional, Intermittent, Frequent and Constant. We want to be able to show that the intensity of pain changed from one number to another, and the frequency improved from 95% to 90%, for example. The metrics of intensity and frequency should be documented on every visit. Outcome questionnaires are the part of the story that tells us about the patient’s function. After the first visit, though, we don’t need to be that thorough. All we need to document for the subjective complaints on subsequent visits are the Site, Intensity and Frequency of each symptom, and if the symptom radiates. This should only take SECONDS to document. The outcome questionnaires should be done every 30 days or sooner, according to Medicare, but it’s even better if we re-assess our patients with these questionnaires every two weeks. For our daily “objective” findings, we only need to follow the P.A.R.T. format that Medicare requires. It’s actually really easy to document, so let’s do it for ALL of our patients. We’ve already hit the requirement for the P of P.A.R.T., which is Pain/Tenderness, in the subjective part of our SOAP note. The A of P.A.R.T. stands for Asymmetry/Misalignment, which includes documentation of spinal and/or extremity restrictions (subluxations), posture and gait. If we document the restrictions on every visit, documenting posture and/or gait are optional. All we need to document for the restrictions are the specific segments, like C4, T5 and so on, and left shoulder, right wrist, etc. This should take all of a few seconds to document. No big deal. The “R” of P.A.R.T. stands for Range of Motion Abnormality. If you want to actually measure range of motion (dual inclinometers for spine, goniometer for extremities), this only needs to be done every 30 days. If you want to assess range of motion on each visit, we only need to document if there is an increase in pain or not with each plane of motion. We can also document if there appears to be diminished or restricted motion in each plane, without measuring it or making up a number. The “T” of P.A.R.T. stands for Tissue/Tone. For this, we only need to document muscle spasms and/or trigger points. Instead of documenting the infamous “paraspinal muscles,” though, it’s much better to document the specific muscles, like “left supraspinatus muscle.” That covers the Subjective and Objective part of our S.O.A.P. note. While the metrics for pain intensity and frequency may change on each visit (but not necessarily), the A, R and T of P.A.R.T. may stay the same for a little while. Change them as they change. So, when we think of “telling the story” for each patient encounter, let’s think in terms of a “short story.” Documentation can be easy and exceptional and fast. We just need to know how to justify. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
Documenting Treatment Goals
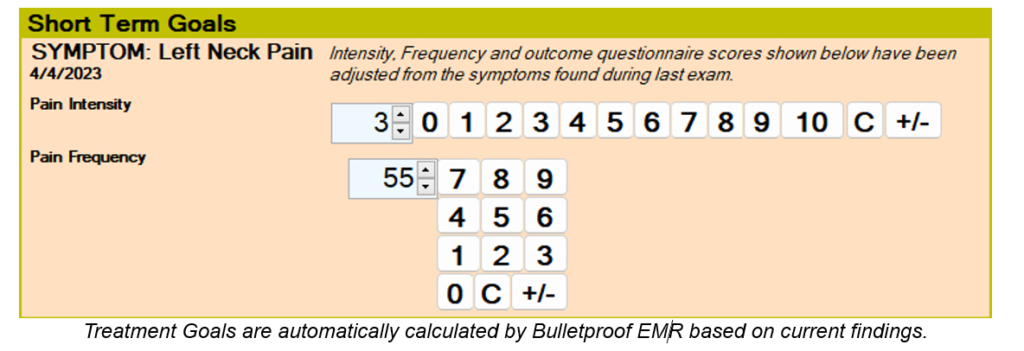
Documenting treatment goals has been an issue for many chiropractors for years. For the few chiropractors who have made the effort, typical goals tend to be things like “reduce pain, reduce muscle spasm, improve range of motion,” regardless of the conditions being treated. When focusing on the Problem Oriented Medical Record format of documentation, which has been the standard since 1968, if we’re treating a patient for headaches, neck pain and low back pain, we should have goals for the headaches, goals for the neck pain and goals for the low back pain. In addition, our goals have to be measurable. In other words, saying “reduce pain” isn’t good enough. We need to say something like, “reduce pain from a 7 to a 5,” or “reduce pain by x%.” Most of you reading this just got nauseous. The next question is, what goals are most relevant to what we do as chiropractors and can be easily calculated and documented? Medicare has been telling us for years that they want to see TWO things from chiropractors: Pain Assessment and Functional Outcome Assessment. It’s not just Medicare who wants this from us now – the entire health-care universe is asking for it, too. And to be perfectly honest, we should be embracing this instead of fearing it. Why? Because we all know how GREAT chiropractic treatment is at improving BOTH pain and function. Why not SHOW it? Let’s talk about pain assessment first. There are quite a few published studies that recommend the Numeric Rating Scale (NRS) and the Visual Analogue Scale (VAS). I’ve used both over the years, and I find the NRS is easier for most patients and doctors. This can be done verbally, as opposed to written (Verbal Numeric Rating Scale [VNRS]). The FREQUENCY of the pain is very often overlooked, though, and is a great metric to track and is easily converted to a goal. This works well when we document the frequency in 5-10% increments of time, such as 25%, 50%, 85%, etc. It does not work well when documenting ranges like Occasional, Intermittent, Frequent and Constant. These two metrics of Pain Intensity and Pain Frequency should be documented for each condition being treated and on every visit. It should only take a few seconds to ask the patient and document their answers. The next metric for the patient’s subjective complaints is the functional outcome assessment. According to CMS (Centers for Medicare and Medicaid Services), this needs to be performed every 30 days or sooner. These work even better if we have the patients complete these every two weeks since it helps us determine quickly if we’re on the right track with the patient or if we need to change the treatment in some way. The fourth metric, which falls under the Objective part of our SOAP note and is optional, are range of motion measurements. Range of motion only serves as an outcome assessment if it’s actually measured, though, not visually estimated by the doctor. This outcome assessment (again, it’s optional), should be performed every 30 days. Just know that the quantity of motion isn’t always clinically relevant. Now that we know which metrics to track (pain intensity, pain frequency, functional outcome questionnaires and range of motion measurements), what should the measurable goals be? According to several published studies, to be considered “clinically significant,” we want to show at least 30% improvement in any of the outcome assessments over a four-week trial of care. You don’t need to show 30% improvement in ALL of the metrics, just one or more. If we’re tracking 3 metrics (pain intensity, pain frequency and functional outcome questionnaires), we have a much better chance of reaching this goal in at least one of these. Some of you are MAD now. “Thirty percent? That’s a LOT!” you may be thinking. It’s not as bad as you think. For example, if the pain intensity is a 7/10, a 30% improvement is a 5/10. Do you think you have a pretty good chance of achieving this within 30 days? If the pain frequency is 80% of awake time, a 30% improvement would be 56% of awake time. If the functional outcome questionnaire score is a 52, a 30% improvement is a 35. As the metrics improve, the 30% mark gets even easier to achieve. For example, if the pain intensity is a 4/10, a 30% improvement is a 3/10 (rounded up from 2.8). See how this works? If you want to figure out a way to calculate these goals manually, it’s certainly doable, but will take a bit of time. This is where technology can help us immensely. In my EMR, I have the program automatically calculate the 30% goal for each metric and it documents it for me. As each metric changes, the goal changes. Chiropractic is awesome. We all know it deep in our souls. Now it’s time to show it. Here are some references you can check out: Younger J, McCue R, Mackey S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep. 2009;13(1):39–43. doi:10.1007/s11916-009-0009-x Clinical versus statistical significance in the assessment of pain relief. Todd KH Ann Emerg Med. 1996 Apr; 27(4):439-41. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM Pain. 2001 Nov; 94(2):149-58. Clinically important changes in acute pain outcome measures: a validation study. Farrar JT, Berlin JA, Strom BL J Pain Symptom Manage. 2003 May; 25(5):406-11. How many repeated measures in repeated measures designs? Statistical issues for comparative trials. Vickers AJ BMC Med Res Methodol. 2003 Oct 27; 3():22. Documentation can be easy and exceptional and fast. We just need to know how to justify. Gregg Friedman, DC, CCSP, FIACA Creator of The Bulletproof Chiro EMR
